

Implementation and Operational Research: Effects of CD4 Monitoring Frequency on Clinical End Points in Clinically Stable HIV-Infected Patients With Viral Suppression
- PMID: 25850606
- PMCID: PMC4506699
- DOI: 10.1097/QAI.0000000000000634
Implementation and Operational Research: Effects of CD4 Monitoring Frequency on Clinical End Points in Clinically Stable HIV-Infected Patients With Viral Suppression
Abstract
Background: Current treatment guidelines for HIV infection recommend routine CD4 lymphocyte (CD4) count monitoring in patients with viral suppression. This may have a limited impact on influencing care as clinically meaningful CD4 decline rarely occurs during viral suppression.
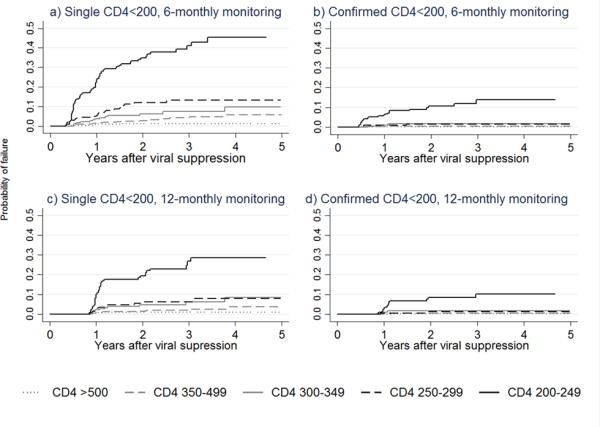
Methods: In a regional HIV observational cohort in the Asia-Pacific region, patients with viral suppression (2 consecutive viral loads <400 copies/mL) and a CD4 count ≥200 cells per microliter who had CD4 testing 6 monthly were analyzed. Main study end points were occurrence of 1 CD4 count <200 cells per microliter (single CD4 <200) and 2 CD4 counts <200 cells per microliter within a 6-month period (confirmed CD4 <200). A comparison of time with single and confirmed CD4 <200 with biannual or annual CD4 assessment was performed by generating a hypothetical group comprising the same patients with annual CD4 testing by removing every second CD4 count.
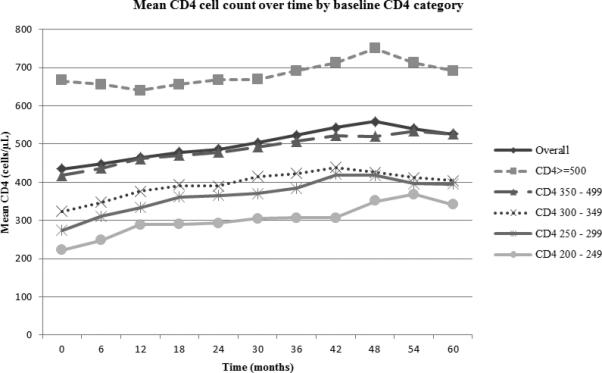
Results: Among 1538 patients, the rate of single CD4 <200 was 3.45/100 patient-years and of confirmed CD4 <200 was 0.77/100 patient-years. During 5 years of viral suppression, patients with baseline CD4 200-249 cells per microliter were significantly more likely to experience confirmed CD4 <200 compared with patients with higher baseline CD4 [hazard ratio, 55.47 (95% confidence interval: 7.36 to 418.20), P < 0.001 versus baseline CD4 ≥500 cells/μL]. Cumulative probabilities of confirmed CD4 <200 was also higher in patients with baseline CD4 200-249 cells per microliter compared with patients with higher baseline CD4. There was no significant difference in time to confirmed CD4 <200 between biannual and annual CD4 measurement (P = 0.336).
Conclusions: Annual CD4 monitoring in virally suppressed HIV patients with a baseline CD4 ≥250 cells per microliter may be sufficient for clinical management.
Figures
References
-
- Egger M, May M, Chene G, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet. 2002;360:119–129. - PubMed
-
- Mellors JW, Munoz A, Giorgi JV, et al. Plasma viral load and CD4+ lymphocytes as prognostic markers of HIV-1 infection. Ann Intern Med. 1997;126:946–954. - PubMed
-
- Battegay M, Nuesch R, Hirschel B, et al. Immunological recovery and antiretroviral therapy in HIV-1 infection. Lancet Infect Dis. 2006;6:280–287. - PubMed
-
- Maggiolo F, Leone S. CD4+ T lymphocyte recovery in individuals with type 1 human immunodeficiency virus infection. Clin Infect Dis. 2010;51:465–467. - PubMed
-
- Garcia F, de Lazzari E, Plana M, et al. Long-term CD4+ T-cell response to highly active antiretroviral therapy according to baseline CD4+ T-cell count. J Acquir Immune Defic Syndr. 2004;36:702–713. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
