

Phase I Hepatic Immunotherapy for Metastases Study of Intra-Arterial Chimeric Antigen Receptor-Modified T-cell Therapy for CEA+ Liver Metastases
- PMID: 25850950
- PMCID: PMC4506253
- DOI: 10.1158/1078-0432.CCR-14-1421
Phase I Hepatic Immunotherapy for Metastases Study of Intra-Arterial Chimeric Antigen Receptor-Modified T-cell Therapy for CEA+ Liver Metastases
Abstract
Purpose: Chimeric antigen receptor-modified T cells (CAR-T) have demonstrated encouraging results in early-phase clinical trials. Successful adaptation of CAR-T technology for CEA-expressing adenocarcinoma liver metastases, a major cause of death in patients with gastrointestinal cancers, has yet to be achieved. We sought to test intrahepatic delivery of anti-CEA CAR-T through percutaneous hepatic artery infusions (HAIs).
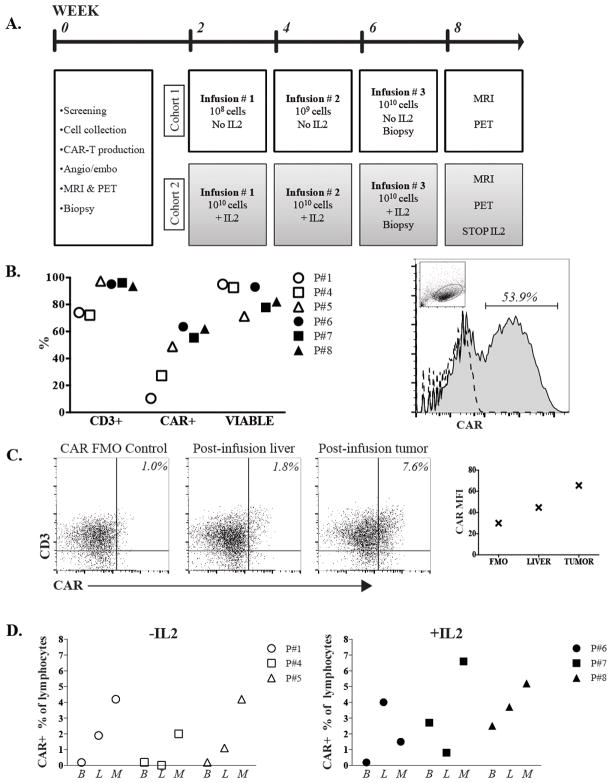
Experimental design: We conducted a phase I trial to test HAI of CAR-T in patients with CEA(+) liver metastases. Six patients completed the protocol, and 3 received anti-CEA CAR-T HAIs alone in dose-escalation fashion (10(8), 10(9), and 10(10) cells). We treated an additional 3 patients with the maximum planned CAR-T HAI dose (10(10) cells × 3) along with systemic IL2 support.
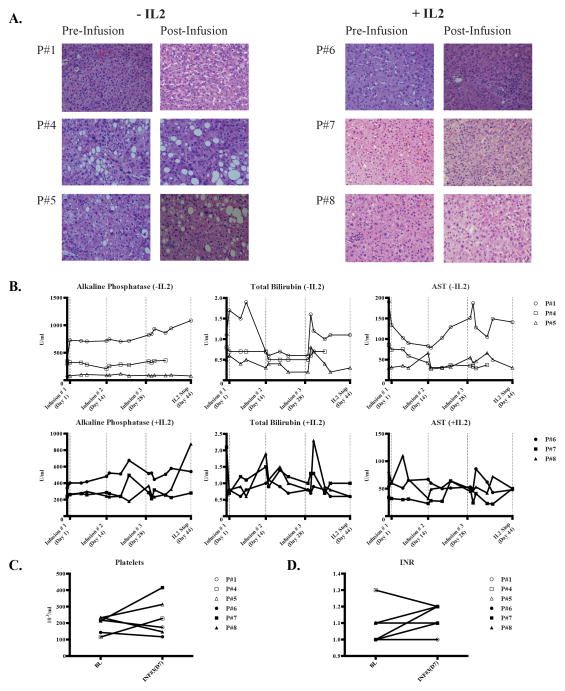
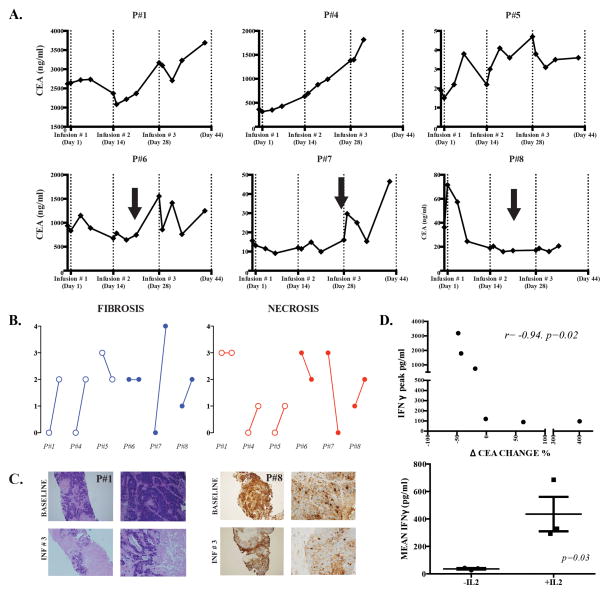
Results: Four patients had more than 10 liver metastases, and patients received a mean of 2.5 lines of conventional systemic therapy before enrollment. No patient suffered a grade 3 or 4 adverse event related to the CAR-T HAIs. One patient remains alive with stable disease at 23 months following CAR-T HAI, and 5 patients died of progressive disease. Among the patients in the cohort that received systemic IL2 support, CEA levels decreased 37% (range, 19%-48%) from baseline. Biopsies demonstrated an increase in liver metastasis necrosis or fibrosis in 4 of 6 patients. Elevated serum IFNγ levels correlated with IL2 administration and CEA decreases.
Conclusions: We have demonstrated the safety of anti-CEA CAR-T HAIs with encouraging signals of clinical activity in a heavily pretreated population with large tumor burdens. Further clinical testing of CAR-T HAIs for liver metastases is warranted.
©2015 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Katz SC, Pillarisetty V, Bamboat ZM, Shia J, Hedvat C, Gonen M, et al. T cell infiltrate predicts long-term survival following resection of colorectal cancer liver metastases. Annals of surgical oncology. 2009;16:2524–30. - PubMed
-
- Wagner P, Koch M, Nummer D, Palm S, Galindo L, Autenrieth D, et al. Detection and functional analysis of tumor infiltrating T-lymphocytes (TIL) in liver metastases from colorectal cancer. Annals of surgical oncology. 2008;15:2310–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
