

Phenotypic clusters within sepsis-associated multiple organ dysfunction syndrome
- PMID: 25851384
- PMCID: PMC4607311
- DOI: 10.1007/s00134-015-3764-7
Phenotypic clusters within sepsis-associated multiple organ dysfunction syndrome
Abstract
Introduction: Sepsis is a devastating condition that is generally treated as a single disease. Identification of meaningfully distinct clusters may improve research, treatment and prognostication among septic patients. We therefore sought to identify clusters among patients with severe sepsis or septic shock.
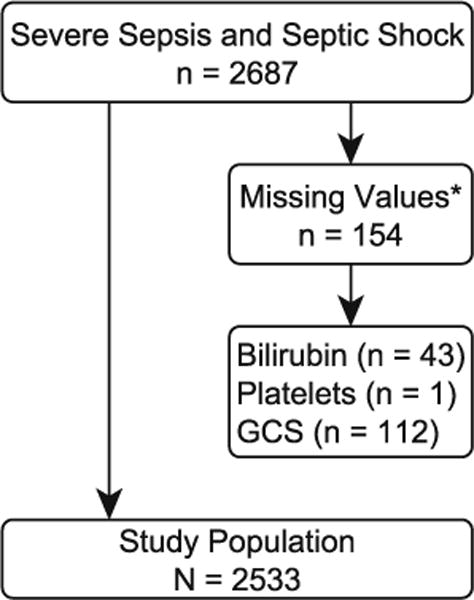
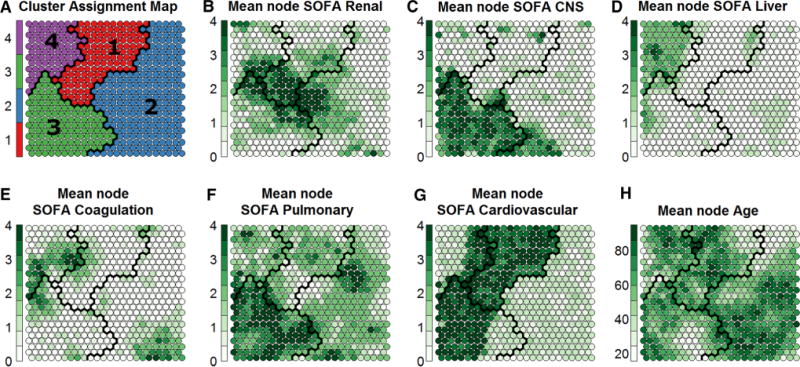
Methods: We retrospectively studied all patients with severe sepsis or septic shock admitted directly from the emergency department to the intensive care units (ICUs) of three hospitals, 2006-2013. Using age and Sequential Organ Failure Assessment (SOFA) subscores, we defined clusters utilizing self-organizing maps, a method for representing multidimensional data in intuitive two-dimensional grids to facilitate cluster identification.
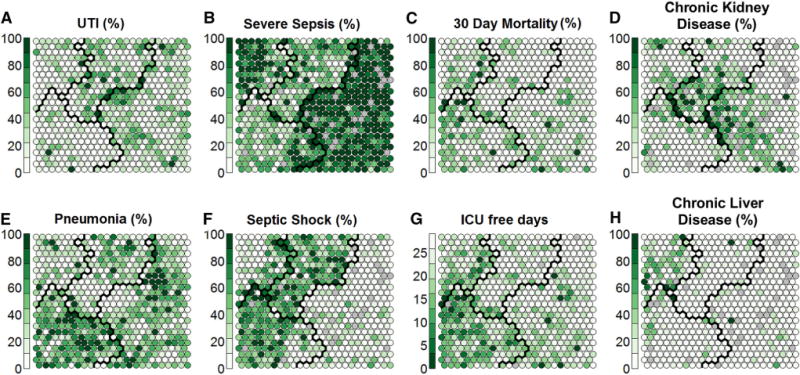
Results: We identified 2533 patients with severe sepsis or septic shock. Overall mortality was 17 %, with a mean APACHE II score of 24, mean SOFA score of 8 and a mean ICU stay of 5.4 days. Four distinct clusters were identified; (1) shock with elevated creatinine, (2) minimal multi-organ dysfunction syndrome (MODS), (3) shock with hypoxemia and altered mental status, and (4) hepatic disease. Mortality (95 % confidence intervals) for these clusters was 11 (8-14), 12 (11-14), 28 (25-32), and 21 (16-26) %, respectively (p < 0.0001). Regression modeling demonstrated that the clusters differed in the association between clinical outcomes and predictors, including APACHE II score.
Conclusions: We identified four distinct clusters of MODS among patients with severe sepsis or septic shock. These clusters may reflect underlying pathophysiological differences and could potentially facilitate tailored treatments or directed research.
Conflict of interest statement
Figures
Comment in
-
Personalized medicine, endotypes, and intensive care medicine.Intensive Care Med. 2015 Jun;41(6):1138-40. doi: 10.1007/s00134-015-3812-3. Epub 2015 Apr 24. Intensive Care Med. 2015. PMID: 25904185 No abstract available.
References
-
- Vincent JL, Moreno R, Takala J, Willatts S, De Mendonca A, Bruining H, Reinhart CK, Suter PM, Thijs LG. The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure. On behalf of the Working group on sepsis-related problems of the European society of intensive care medicine. Intensive Care Med. 1996;22:707–710. - PubMed
-
- Vincent JL, Sakr Y, Sprung CL, Ranieri VM, Reinhart K, Gerlach H, Moreno R, Carlet J, Le Gall JR, Payen D. Sepsis occurrence in acutely Ill patients I, sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006;34:344–353. - PubMed
-
- Leligdowicz A, Dodek PM, Norena M, Wong H, Kumar A, Kumar A, Cooperative antimicrobial therapy of septic shock database research G Association between source of infection and hospital mortality in patients who have septic shock. Am J Respir Crit Care Med. 2014;189:1204–1213. - PubMed
-
- Howell MD, Talmor D, Schuetz P, Hunziker S, Jones AE, Shapiro NI. Proof of principle: the predisposition, infection, response, organ failure sepsis staging system. Crit Care Med. 2011;39:322–327. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
