

Circulating tumor DNA as an early marker of therapeutic response in patients with metastatic colorectal cancer
- PMID: 25851626
- PMCID: PMC4511218
- DOI: 10.1093/annonc/mdv177
Circulating tumor DNA as an early marker of therapeutic response in patients with metastatic colorectal cancer
Abstract
Background: Early indicators of treatment response in metastatic colorectal cancer (mCRC) could conceivably be used to optimize treatment. We explored early changes in circulating tumor DNA (ctDNA) levels as a marker of therapeutic efficacy.
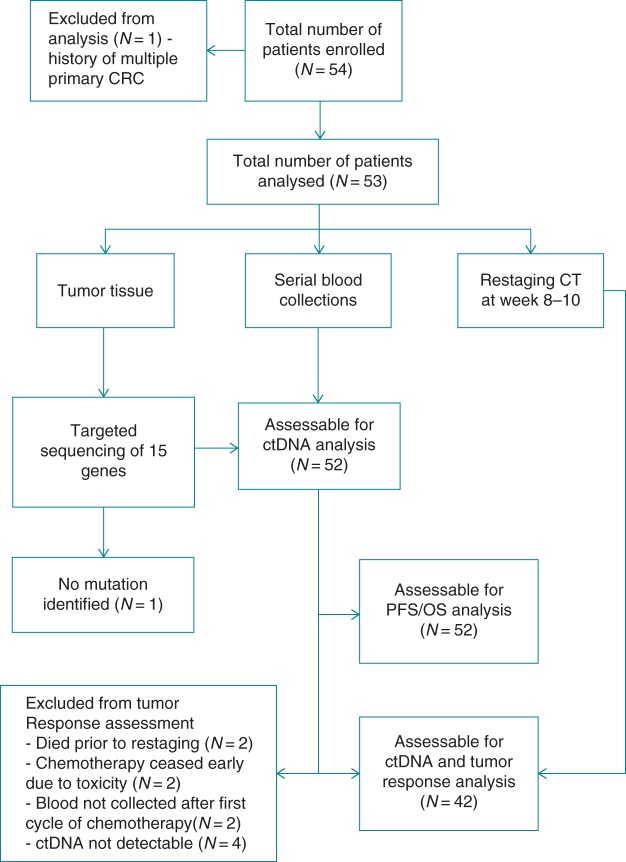
Patients and methods: This prospective study involved 53 mCRC patients receiving standard first-line chemotherapy. Both ctDNA and CEA were assessed in plasma collected before treatment, 3 days after treatment and before cycle 2. Computed tomography (CT) scans were carried out at baseline and 8-10 weeks and were centrally assessed using RECIST v1.1 criteria. Tumors were sequenced using a panel of 15 genes frequently mutated in mCRC to identify candidate mutations for ctDNA analysis. For each patient, one tumor mutation was selected to assess the presence and the level of ctDNA in plasma samples using a digital genomic assay termed Safe-SeqS.
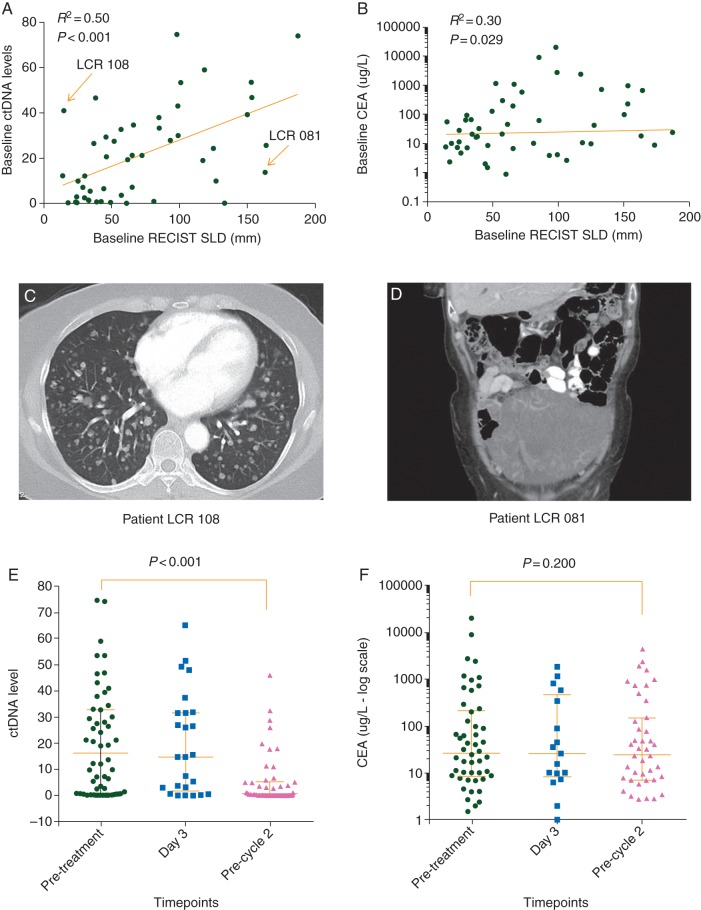
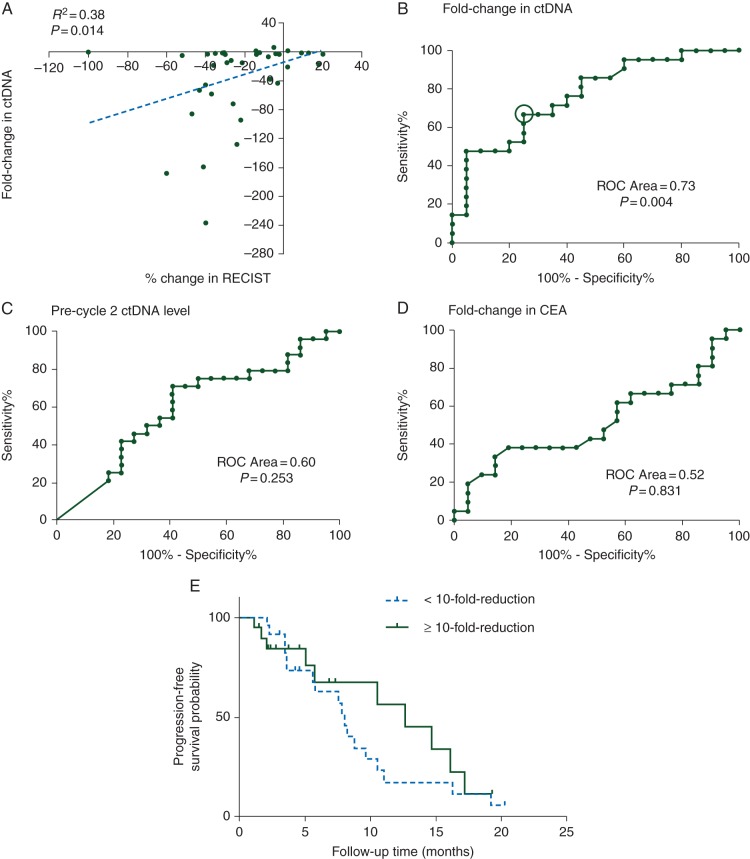
Results: Candidate mutations for ctDNA analysis were identified in 52 (98.1%) of the tumors. These patient-specific candidate tissue mutations were detectable in the cell-free DNA from the plasma of 48 of these 52 patients (concordance 92.3%). Significant reductions in ctDNA (median 5.7-fold; P < 0.001) levels were observed before cycle 2, which correlated with CT responses at 8-10 weeks (odds ratio = 5.25 with a 10-fold ctDNA reduction; P = 0.016). Major reductions (≥10-fold) versus lesser reductions in ctDNA precycle 2 were associated with a trend for increased progression-free survival (median 14.7 versus 8.1 months; HR = 1.87; P = 0.266).
Conclusions: ctDNA is detectable in a high proportion of treatment naïve mCRC patients. Early changes in ctDNA during first-line chemotherapy predict the later radiologic response.
Keywords: biomarker; circulating tumor DNA; metastatic colorectal cancer; treatment response.
© The Author 2015. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Liquid biopsies to evaluate early therapeutic response in colorectal cancer.Ann Oncol. 2015 Aug;26(8):1525-7. doi: 10.1093/annonc/mdv228. Epub 2015 May 12. Ann Oncol. 2015. PMID: 25969369 No abstract available.
References
-
- Ferlay J, Soerjomataram I, Ervik M et al. GLOBOCAN 2012 v1.0—cancer incidence and mortality worldwide: IARC CancerBase No. 11. [Internet] Lyon, France: International Agency for Research on Cancer, 2013; http://globocan.iarc.fr (17 March 2015, date last accessed).
-
- Sharma MR, Maitland ML, Ratain MJ. RECIST: no longer the sharpest tool in the oncology clinical trials toolbox. Cancer Res 2012; 72: 5145–5149. - PubMed
-
- Bast RC Jr, Ravdin P, Hayes DF et al. 2000 update of recommendations for the use of tumor markers in breast and colorectal cancer: clinical practice guidelines of the American Society of Clinical Oncology. J Clin Oncol 2001; 19: 1865–1878. - PubMed
-
- Sorbye H, Dahl O. Carcinoembryonic antigen surge in metastatic colorectal cancer patients responding to oxaliplatin combination chemotherapy: implications for tumor marker monitoring and guidelines. J Clin Oncol 2003; 21: 4466–4467. - PubMed
-
- Goldstein MJ, Mitchell EP. Carcinoembryonic antigen in the staging and follow-up of patients with colorectal cancer. Cancer Invest 2005; 23: 338–351. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
