

Ubiquitin carboxy-terminal hydrolase-l1 as a serum neurotrauma biomarker for exposure to occupational low-level blast
- PMID: 25852633
- PMCID: PMC4360700
- DOI: 10.3389/fneur.2015.00049
Ubiquitin carboxy-terminal hydrolase-l1 as a serum neurotrauma biomarker for exposure to occupational low-level blast
Abstract
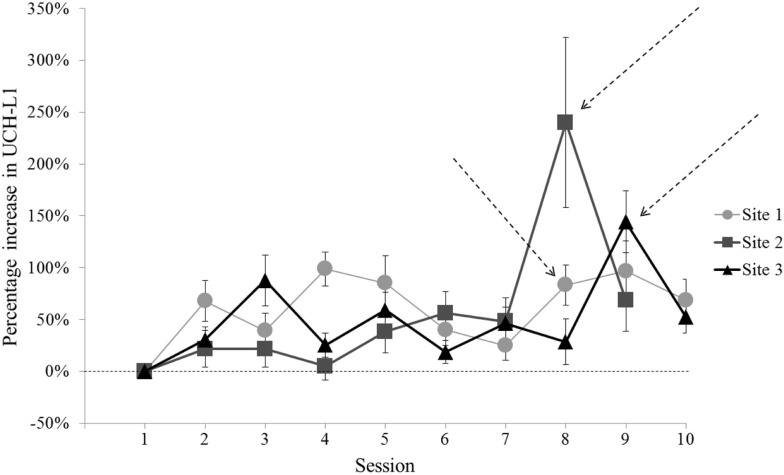
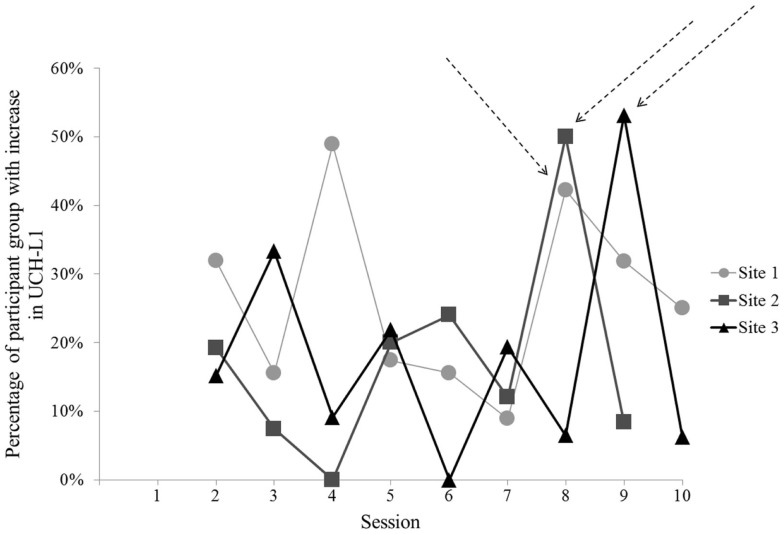
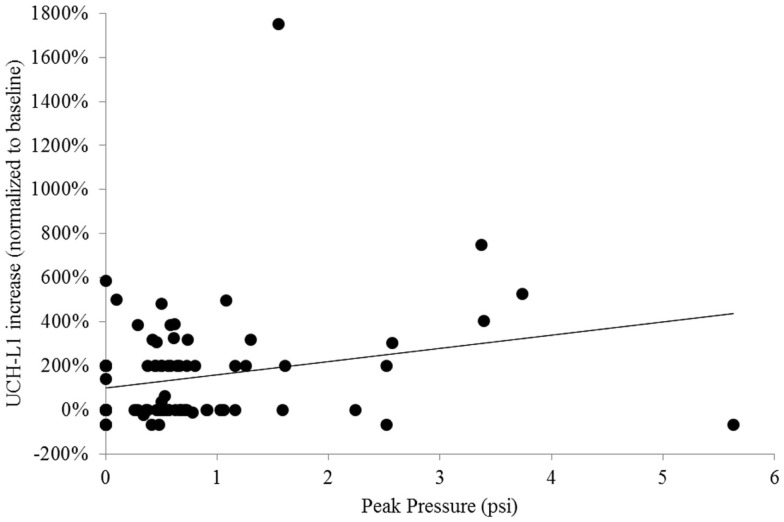
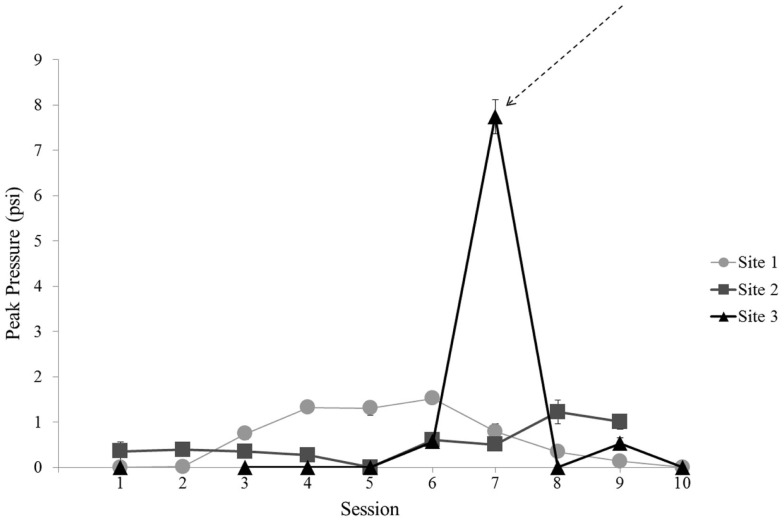
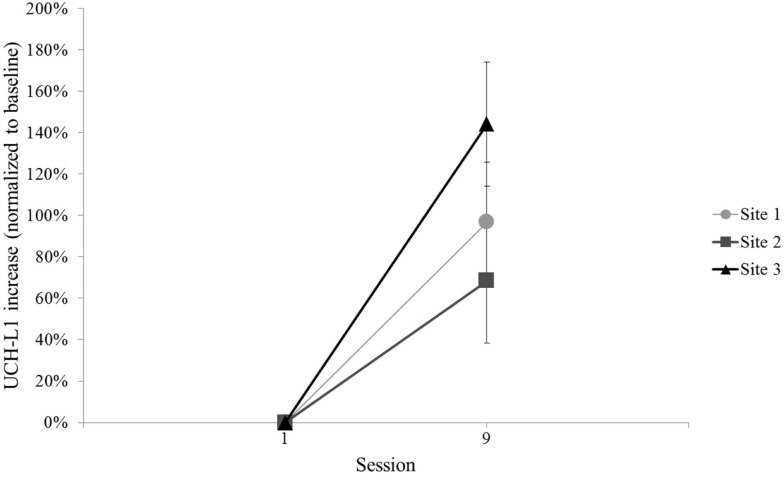
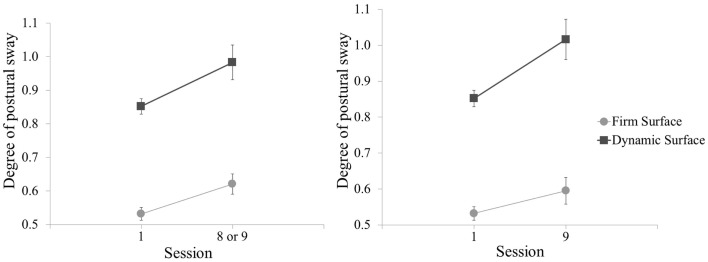
Repeated exposure to low-level blast is a characteristic of a few select occupations and there is concern that such occupational exposures present risk for traumatic brain injury. These occupations include specialized military and law enforcement units that employ controlled detonation of explosive charges for the purpose of tactical entry into secured structures. The concern for negative effects from blast exposure is based on rates of operator self-reported headache, sleep disturbance, working memory impairment, and other concussion-like symptoms. A challenge in research on this topic has been the need for improved assessment tools to empirically evaluate the risk associated with repeated exposure to blast overpressure levels commonly considered to be too low in magnitude to cause acute injury. Evaluation of serum-based neurotrauma biomarkers provides an objective measure that is logistically feasible for use in field training environments. Among candidate biomarkers, ubiquitin carboxy-terminal hydrolase-L1 (UCH-L1) has some empirical support and was evaluated in this study. We used daily blood draws to examine acute change in UCH-L1 among 108 healthy military personnel who were exposed to repeated low-level blast across a 2-week period. These research volunteers also wore pressure sensors to record blast exposures, wrist actigraphs to monitor sleep patterns, and completed daily behavioral assessments of symptomology, postural stability, and neurocognitive function. UCH-L1 levels were elevated as a function of participating in the 2-week training with explosives, but the correlation of UCH-L1 elevation and blast magnitude was weak and inconsistent. Also, UCH-L1 elevations did not correlate with deficits in behavioral measures. These results provide some support for including UCH-L1 as a measure of central nervous system effects from exposure to low-level blast. However, the weak relation observed suggests that additional indicators of blast effect are needed.
Keywords: biomarker; blast; breacher; military; neurotrauma.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous