

How good are we at managing acute kidney injury in hospital?
- PMID: 25852863
- PMCID: PMC4377786
- DOI: 10.1093/ckj/sfu010
How good are we at managing acute kidney injury in hospital?
Abstract
Introduction: Acute kidney injury (AKI) is a common clinical problem associated with adverse outcomes. This study identifies the incidence of AKI in two UK district general hospitals' without on-site renal services and assesses AKI management and level of nephrologist input.
Methods: The AKIN classification was used to identify 1020 AKI patients over 6 months. Data were collated on patient demographics, AKI management and referral to nephrology and intensive care services. Short/long-term renal outcomes were investigated. Patients were followed up for 14 months post-discharge.
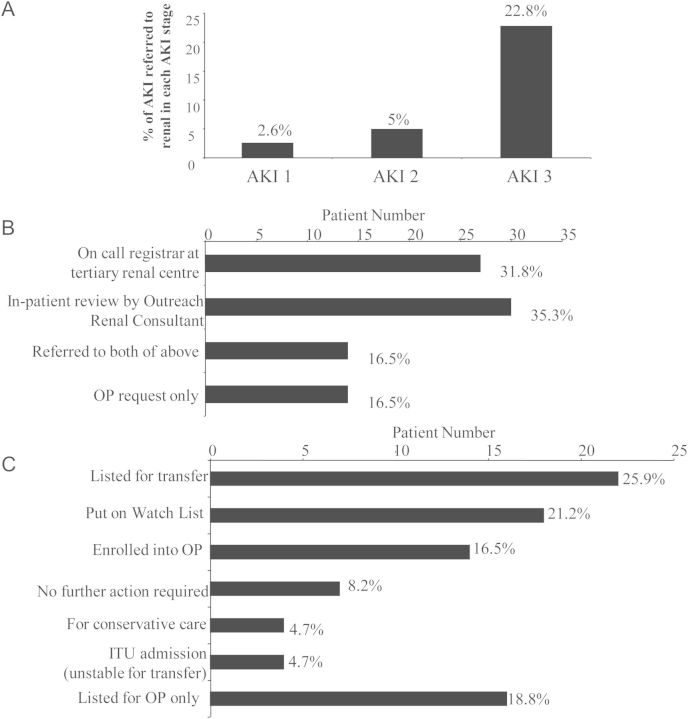
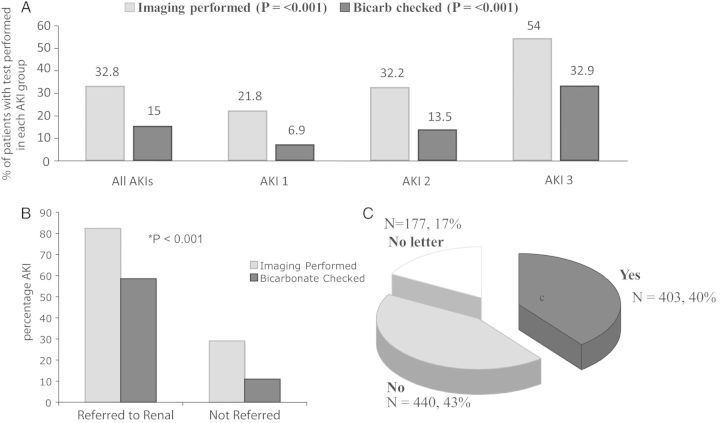
Results: Incidence of hospital-based AKI was 6.4%. Mean patient age was 73 years. There was 28.1% acute in-hospital mortality with a further 21.6% 14-month mortality. Only 8.3% of patients were referred to nephrology services for in-hospital review, and only 8.1% had outpatient nephrology follow-up. Compliance with the AKI National Confidential Enquiry into Patient Outcomes and Deaths (NCEPOD) recommendations was poor with 32.8% of patients having renal imaging and 15% of patients having acid-base status assessed. NCEPOD compliance improved with nephrology input. Patients referred to nephrology were likely to be younger with pre-existing CKD and severe AKI. 10.5% of AKI episodes were unrecognized. Forty percent of those with unrecognized AKI, (compared with 15% of recognized AKI) developed de novo or progression of pre-existing CKD.
Conclusion: AKI in DGHs is mostly managed without nephrology input. There are significant shortcomings in AKI recognition and management in this setting. This is associated with poor mortality and long-term CKD. This study supports a need to improve the teaching and training of front-line medical staff in identifying AKI. Additionally, implementation of AKI e-alert systems may encourage early recognition and provide a prompt for renal referral.
Keywords: acute kidney injury; outcomes.
Figures
References
-
- Aitken E, Carruthers C, Gall L, et al. Acute kidney injury: outcomes and quality of care. QJM. 2013;106:323–332. - PubMed
-
- Ali T, Khan I, Simpson W, et al. Incidence and outcomes in acute kidney injury: a comprehensive population-based study. J Am Soc Nephrol. 2007;18:1292–1298. - PubMed
-
- Chertow GM, Burdick E, Honour M, et al. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16:3365–3370. - PubMed
-
- Waikar SS, Liu KD, Chertow GM. Diagnosis, epidemiology and outcomes of acute kidney injury. Clin J Am Soc Nephrol. 2008;3:844–861. - PubMed
-
- National Confidential Enquiry Into Patient Outcome and Death (NCEPOD) Adding Insult to Injury. London: NCEPOD; 2009.
LinkOut - more resources
Full Text Sources
Other Literature Sources
