

Review of atrophic gastritis and intestinal metaplasia as a premalignant lesion of gastric cancer
- PMID: 25853101
- PMCID: PMC4384712
- DOI: 10.15430/JCP.2015.20.1.25
Review of atrophic gastritis and intestinal metaplasia as a premalignant lesion of gastric cancer
Abstract
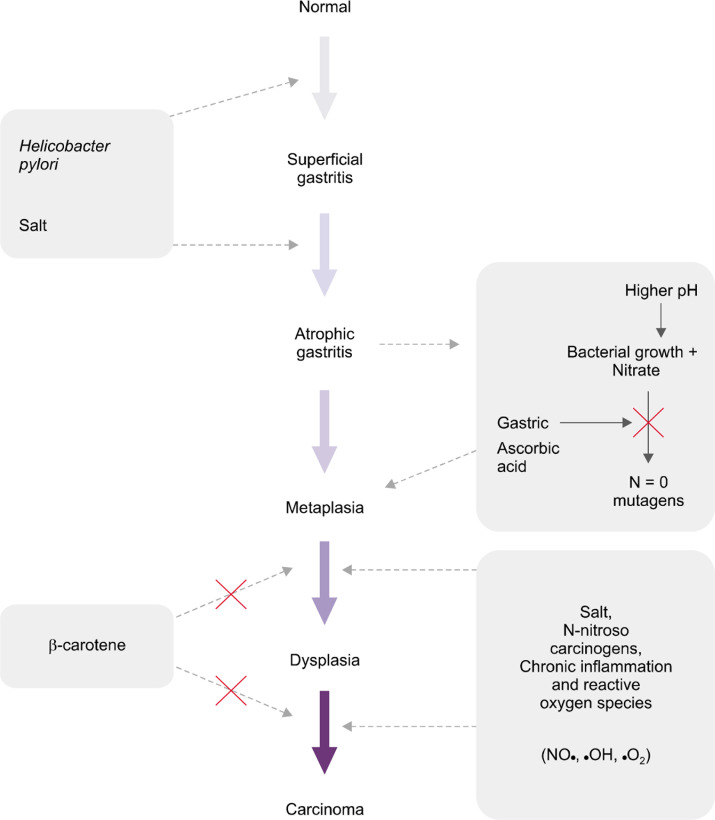
Atrophic gastritis (AG) and intestinal metaplasia (IM) are the main precursor lesions of gastric cancer as the incidence of gastric cancer increases in the gastric mucosa involved with AG and IM. The prevalence of AG and IM vary depending on countries, even it represents diverse results in the same nation. Usually AG is antecedent of IM but the etiologies of AG and IM are not always the same. The sensitivity and specificity of diagnostic methods to detect AG and IM are different. Furthermore, the management strategy of AG and IM has not been established, yet. Helicobacter pylori infection has been proved as the most important cause of AG and IM. Thus the eradication of H. pylori is very important to prevent the progression to gastric cancer which is still placed in the high rank in morbidity and mortality among cancers. However, the reversibility of AG and IM by eradication of H. pylori which was assumed to be certain by meta-analysis is; however, controversial now. Therefore, the understanding and early diagnosis of AG and IM are very important, especially, in high incidence area of gastric cancer such as Republic of Korea.
Keywords: Atrophic gastritis; Gastric cancer; Helicobacter pylori; Intestinal metaplasia.
Figures
References
-
- Statistics Korea. Daejeon, Statistics Korea. 2013 Available from: http://kostat.go.kr. Accessed December 3, 2014.
-
- Hundahl SA, Phillips JL, Menck HR. The National Cancer Data Base Report on poor survival of U.S. gastric carcinoma patients treated with gastrectomy: fifth edition American Joint Committee on Cancer staging, proximal disease, and the “different disease” hypothesis. Cancer. 2000;88:921–32. doi: 10.1002/(SICI)1097-0142(20000215)88:4<921::AID-CNCR24>3.0.CO;2-S. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources