

Phenotype standardization for drug-induced kidney disease
- PMID: 25853333
- PMCID: PMC4758130
- DOI: 10.1038/ki.2015.115
Phenotype standardization for drug-induced kidney disease
Abstract
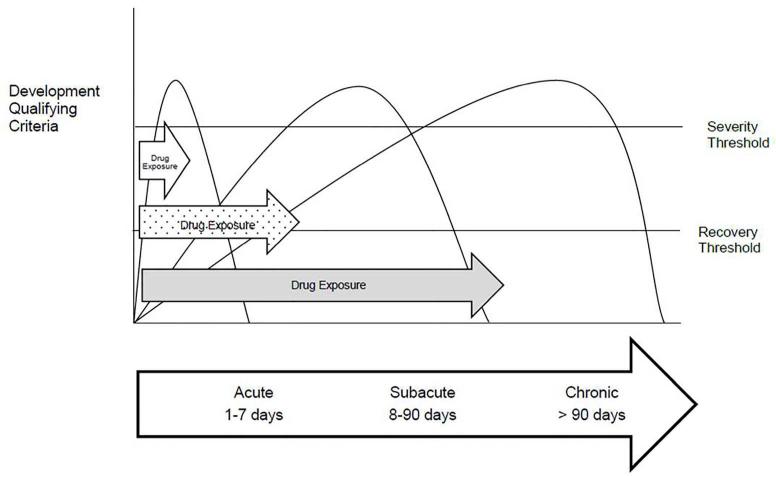
Drug-induced kidney disease is a frequent cause of renal dysfunction; however, there are no standards to identify and characterize the spectrum of these disorders. We convened a panel of international, adult and pediatric, nephrologists and pharmacists to develop standardized phenotypes for drug-induced kidney disease as part of the phenotype standardization project initiated by the International Serious Adverse Events Consortium. We propose four phenotypes of drug-induced kidney disease based on clinical presentation: acute kidney injury, glomerular, tubular, and nephrolithiasis, along with the primary and secondary clinical criteria to support the phenotype definition, and a time course based on the KDIGO/AKIN definitions of acute kidney injury, acute kidney disease, and chronic kidney disease. Establishing causality in drug-induced kidney disease is challenging and requires knowledge of the biological plausibility for the specific drug, mechanism of injury, time course, and assessment of competing risk factors. These phenotypes provide a consistent framework for clinicians, investigators, industry, and regulatory agencies to evaluate drug nephrotoxicity across various settings. We believe that this is the first step to recognizing drug-induced kidney disease and developing strategies to prevent and manage this condition.
Figures
References
-
- Mehta RL, et al. Spectrum of acute renal failure in the intensive care unit: the PICARD experience. Kidney Int. 2004;66(4):1613–21. - PubMed
-
- Aithal GP, et al. Case definition and phenotype standardization in drug-induced liver injury. Clin Pharmacol Ther. 2011;89(6):806–15. - PubMed
-
- Group., K.D.I.G.O.K.A.K.I.W. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter. 2012;2:1–138.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
