

Cerebrospinal fluid cytokine profiles predict risk of early mortality and immune reconstitution inflammatory syndrome in HIV-associated cryptococcal meningitis
- PMID: 25853653
- PMCID: PMC4390200
- DOI: 10.1371/journal.ppat.1004754
Cerebrospinal fluid cytokine profiles predict risk of early mortality and immune reconstitution inflammatory syndrome in HIV-associated cryptococcal meningitis
Abstract
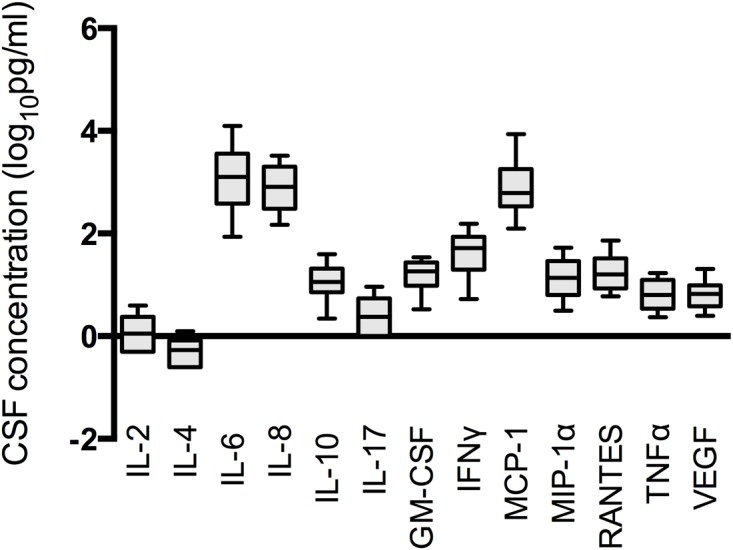
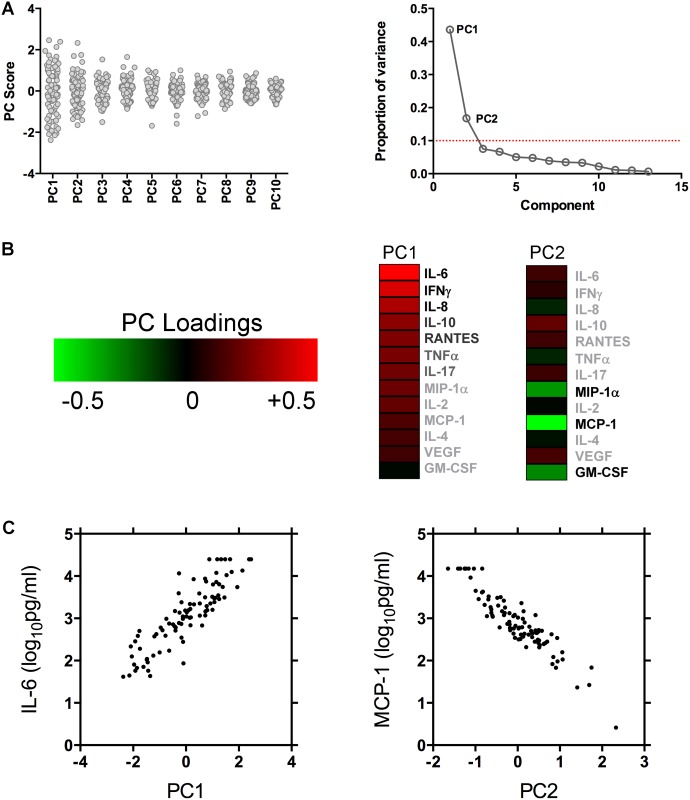
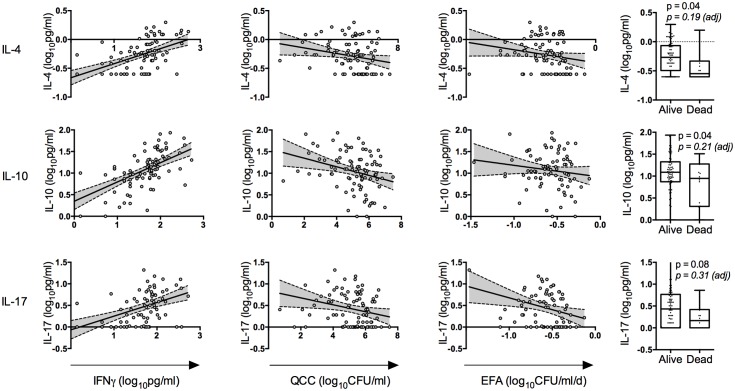
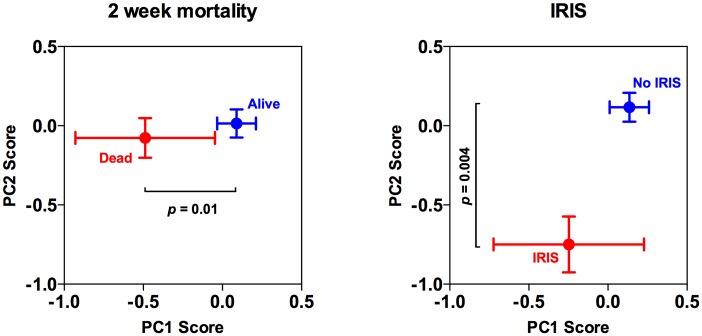
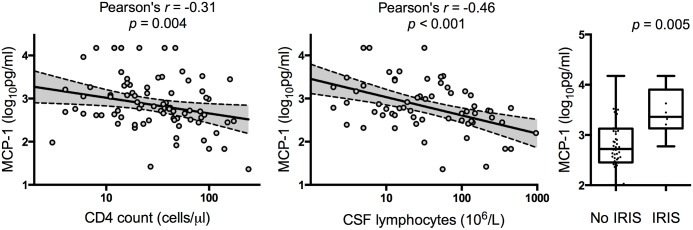
Understanding the host immune response during cryptococcal meningitis (CM) is of critical importance for the development of immunomodulatory therapies. We profiled the cerebrospinal fluid (CSF) immune-response in ninety patients with HIV-associated CM, and examined associations between immune phenotype and clinical outcome. CSF cytokine, chemokine, and macrophage activation marker concentrations were assayed at disease presentation, and associations between these parameters and microbiological and clinical outcomes were examined using principal component analysis (PCA). PCA demonstrated a co-correlated CSF cytokine and chemokine response consisting primarily of Th1, Th2, and Th17-type cytokines. The presence of this CSF cytokine response was associated with evidence of increased macrophage activation, more rapid clearance of Cryptococci from CSF, and survival at 2 weeks. The key components of this protective immune-response were interleukin (IL)-6 and interferon-γ, IL-4, IL-10 and IL-17 levels also made a modest positive contribution to the PC1 score. A second component of co-correlated chemokines was identified by PCA, consisting primarily of monocyte chemotactic protein-1 (MCP-1) and macrophage inflammatory protein-1α (MIP-1α). High CSF chemokine concentrations were associated with low peripheral CD4 cell counts and CSF lymphocyte counts and were predictive of immune reconstitution inflammatory syndrome (IRIS). In conclusion CSF cytokine and chemokine profiles predict risk of early mortality and IRIS in HIV-associated CM. We speculate that the presence of even minimal Cryptococcus-specific Th1-type CD4+ T-cell responses lead to increased recruitment of circulating lymphocytes and monocytes into the central nervous system (CNS), more effective activation of CNS macrophages and microglial cells, and faster organism clearance; while high CNS chemokine levels may predispose to over recruitment or inappropriate recruitment of immune cells to the CNS and IRIS following peripheral immune reconstitution with ART. These results provide a rational basis for future studies of immune modulation in CM, and demonstrate the potential of baseline immune profiling to identify CM patients most at risk of mortality and subsequent IRIS.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: JNJ and TSH have received research support through a Gilead investigator initiated award. TB has served on an advisory board and received support for conference attendance from Gilead. All other authors report no potential conflicts of interest.This does not alter our adherence to all PLOS policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
