

CDKN2A loss is associated with shortened overall survival in lower-grade (World Health Organization Grades II-III) astrocytomas
- PMID: 25853694
- PMCID: PMC4397174
- DOI: 10.1097/NEN.0000000000000188
CDKN2A loss is associated with shortened overall survival in lower-grade (World Health Organization Grades II-III) astrocytomas
Abstract
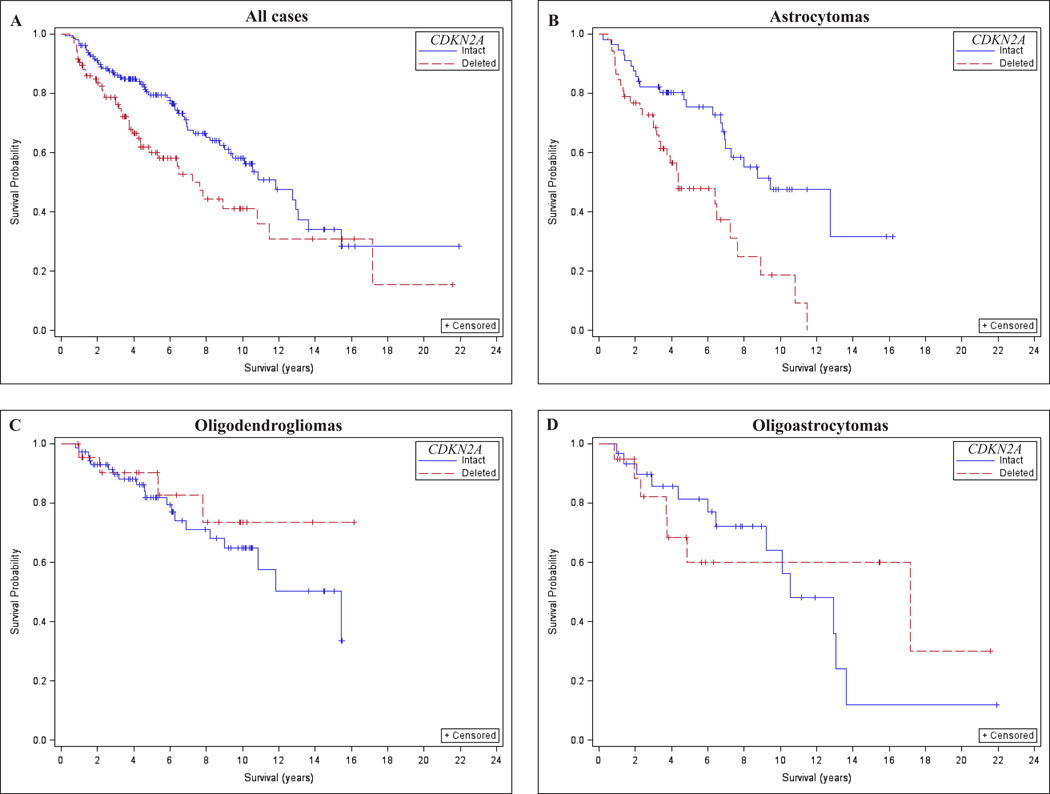
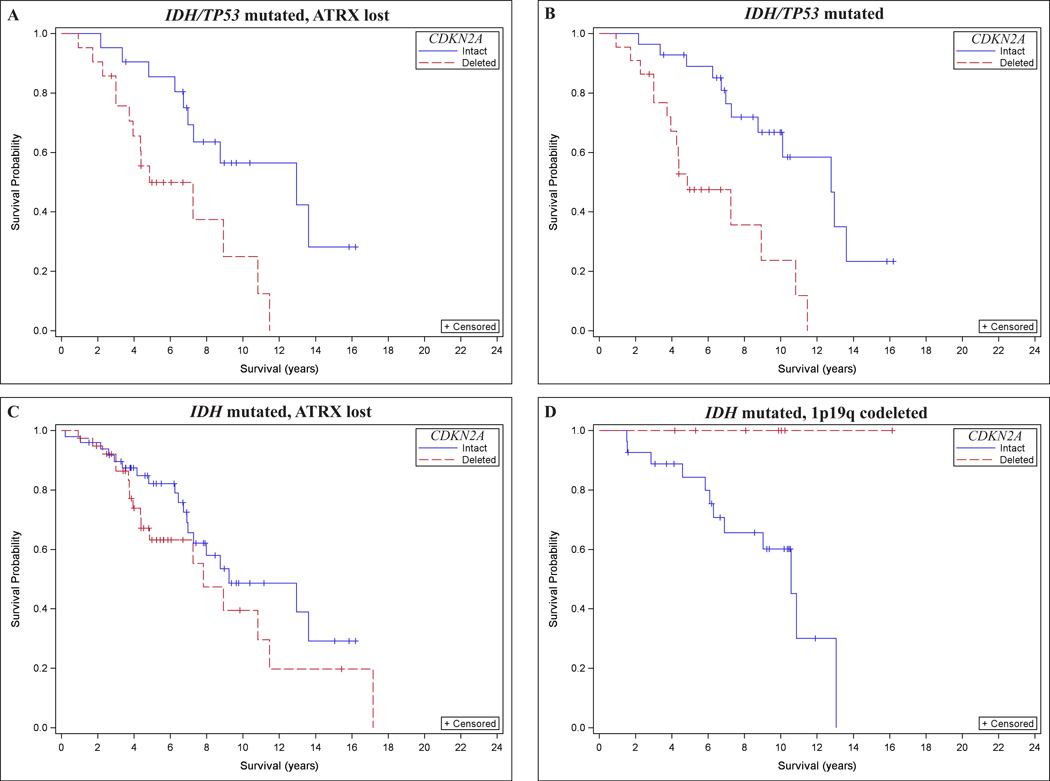
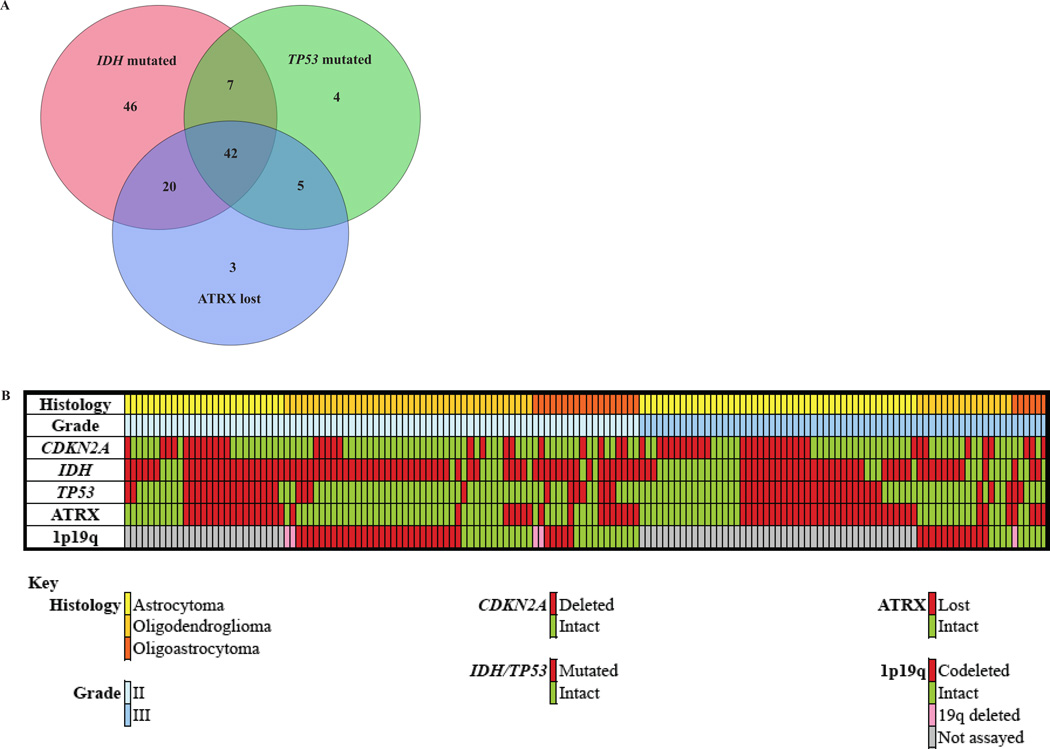
Lower-grade (World Health Organization Grades II and III) gliomas vary widely in clinical behavior and are classified as astrocytic, oligodendroglial, or mixed. Anaplasia depends greatly on mitotic activity, with CDKN2A loss considered as the most common mechanism for cell cycle dysregulation. We investigated whether loss of the CDKN2A gene is associated with overall survival across pathologically and genetically defined glioma subtypes. After adjustment for IDH mutation, sex, and age, CDKN2A deletion was strongly associated with poorer overall survival in astrocytomas but not in oligodendrogliomas or oligoastrocytomas. Molecular classification of astrocytomas by IDH mutation, TP53 mutation, and /or ATRX loss of expression revealed that CDKN2A loss in IDH/TP53 mutated tumors was strongly associated with worse overall survival. CDKN2A loss in IDH mutated tumors with ATRX loss was only weakly associated with worse overall survival. These findings suggest that CDKN2A testing may provide further clinical aid in lower-grade glioma substratification beyond IDH mutation and 1p19q codeletion status, particularly in IDH/TP53 mutated astrocytomas.
Figures
References
-
- Bourne TD, Schiff D. Update on molecular findings, management and outcome in low-grade gliomas. Nat Rev Neurol. 2010;6:695–701. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
