

Urinary tract infections: epidemiology, mechanisms of infection and treatment options
- PMID: 25853778
- PMCID: PMC4457377
- DOI: 10.1038/nrmicro3432
Urinary tract infections: epidemiology, mechanisms of infection and treatment options
Abstract
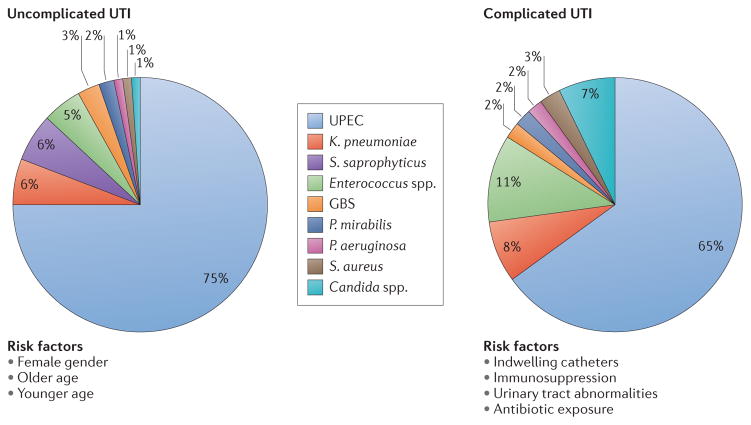
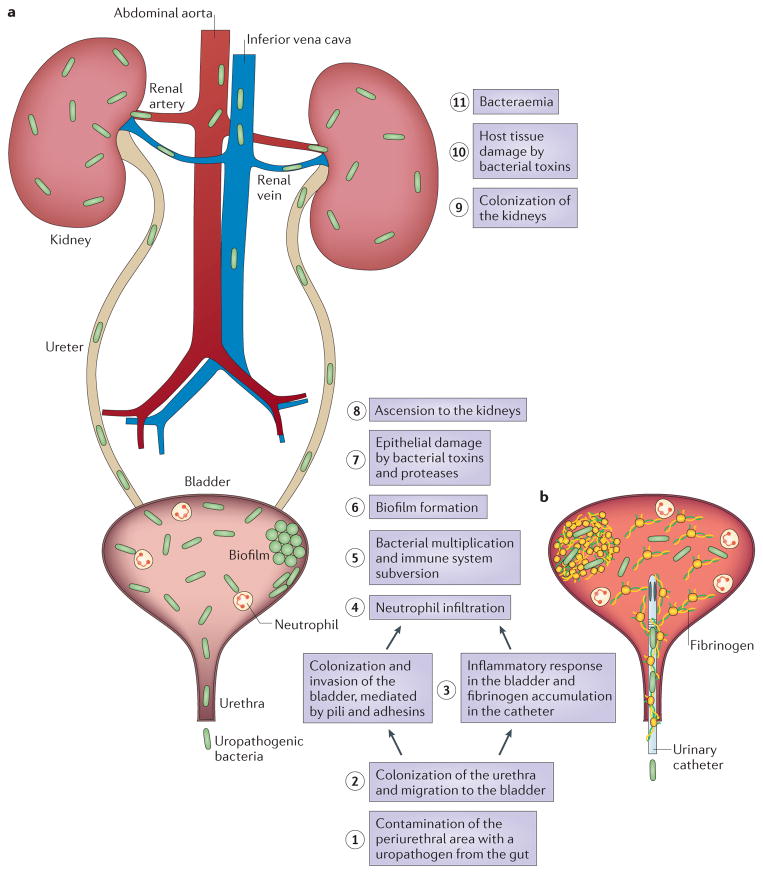
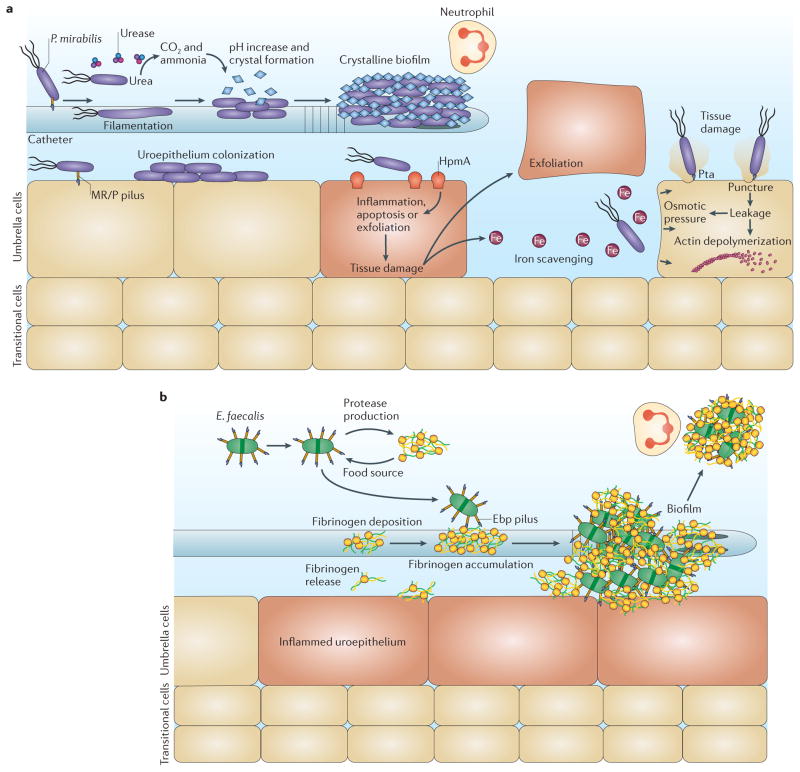
Urinary tract infections (UTIs) are a severe public health problem and are caused by a range of pathogens, but most commonly by Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, Enterococcus faecalis and Staphylococcus saprophyticus. High recurrence rates and increasing antimicrobial resistance among uropathogens threaten to greatly increase the economic burden of these infections. In this Review, we discuss how basic science studies are elucidating the molecular details of the crosstalk that occurs at the host-pathogen interface, as well as the consequences of these interactions for the pathophysiology of UTIs. We also describe current efforts to translate this knowledge into new clinical treatments for UTIs.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Stamm WE, Norrby SR. Urinary tract infections: disease panorama and challenges. J Infect Dis. 2001;183 (Suppl 1):S1–S4. - PubMed
-
- Schappert SM, Rechtsteiner EA. Ambulatory medical care utilization estimates for 2007. Vital Health Stat. 2011;13:1–38. - PubMed
-
- Foxman B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am. 2014;28:1–13. This paper presents the most recent information about UTIs and their socioeconomic impact. - PubMed
-
- Foxman B. The epidemiology of urinary tract infection. Nature Rev Urol. 2010;7:653–660. - PubMed
-
- Hooton TM. Uncomplicated urinary tract infection. New Engl J Med. 2012;366:1028–1037. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
