

Antiplatelet therapy discontinuation and the risk of serious cardiovascular events after coronary stenting: observations from the CREDO-Kyoto Registry Cohort-2
- PMID: 25853836
- PMCID: PMC4390156
- DOI: 10.1371/journal.pone.0124314
Antiplatelet therapy discontinuation and the risk of serious cardiovascular events after coronary stenting: observations from the CREDO-Kyoto Registry Cohort-2
Abstract
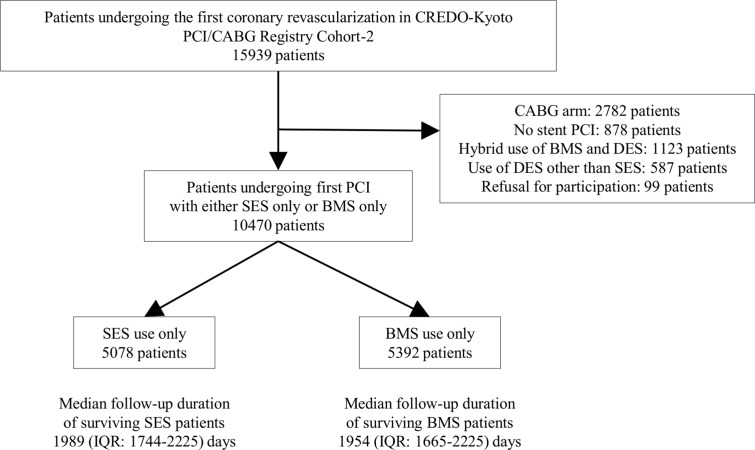
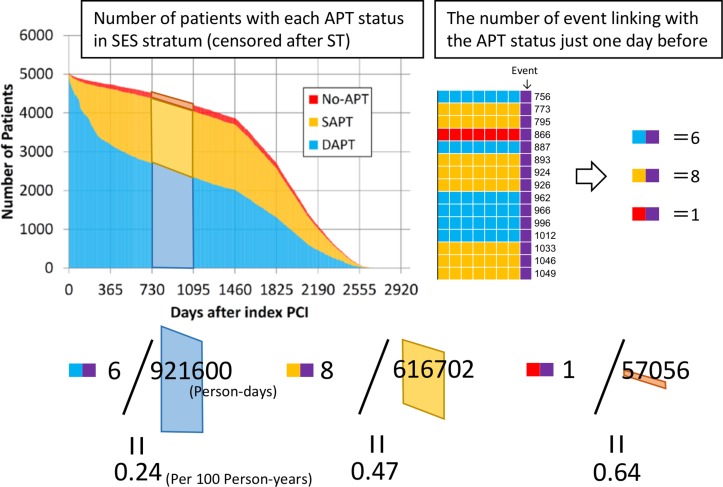
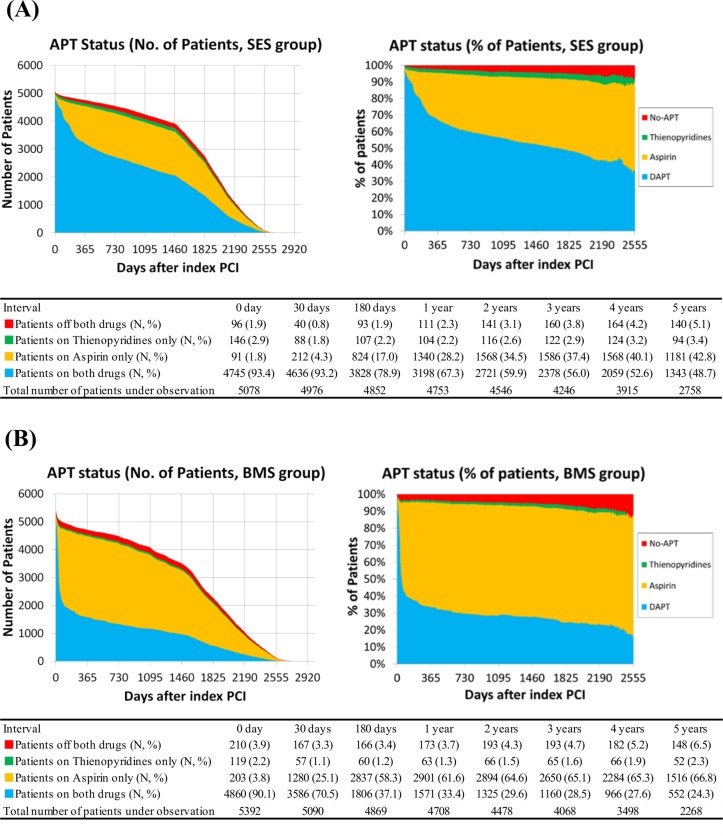
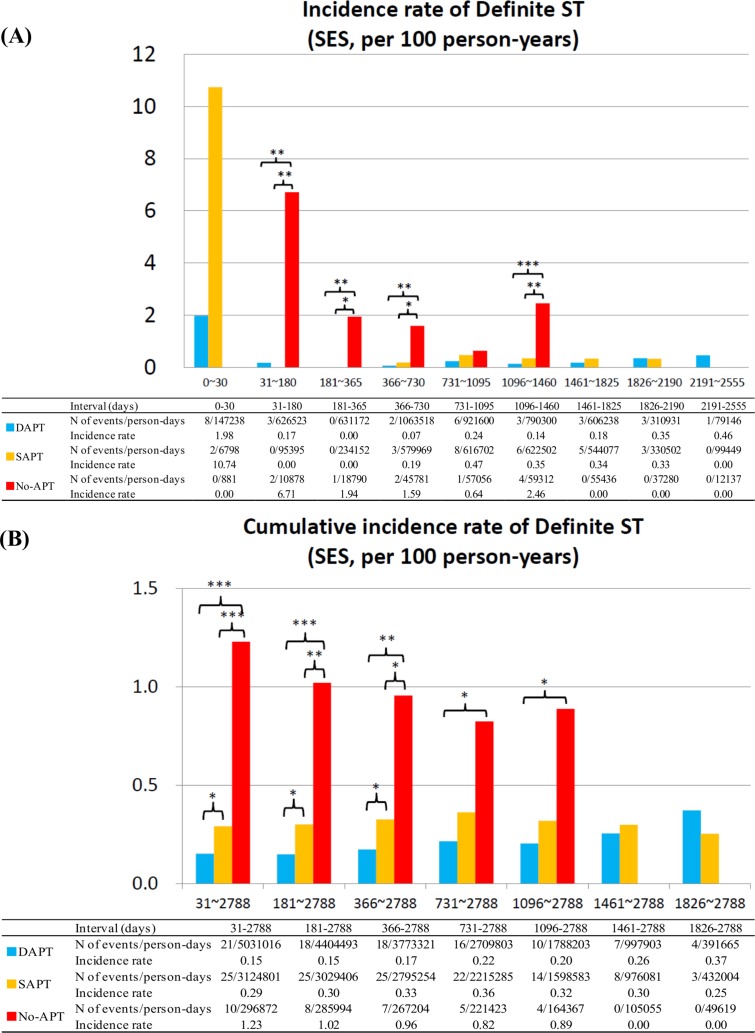
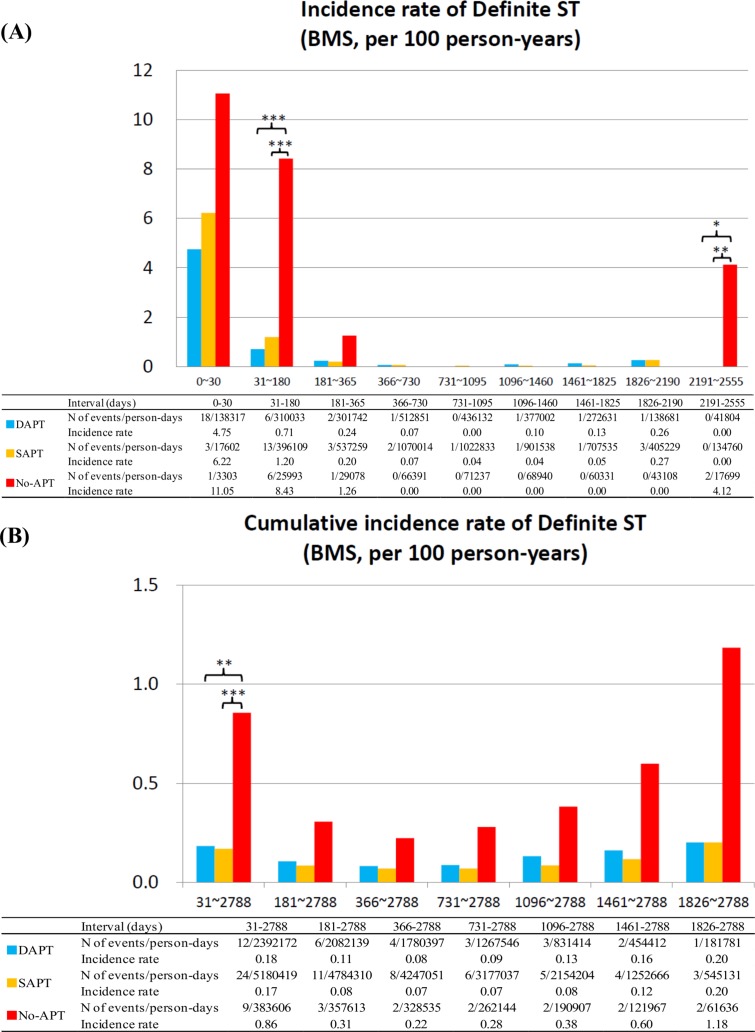
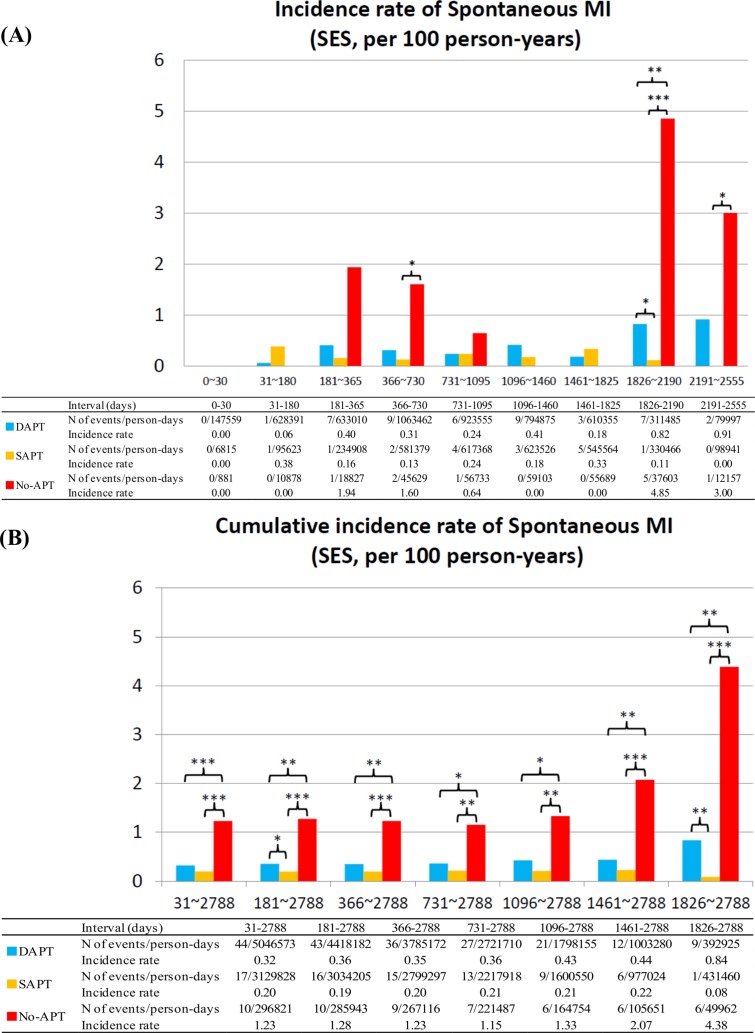
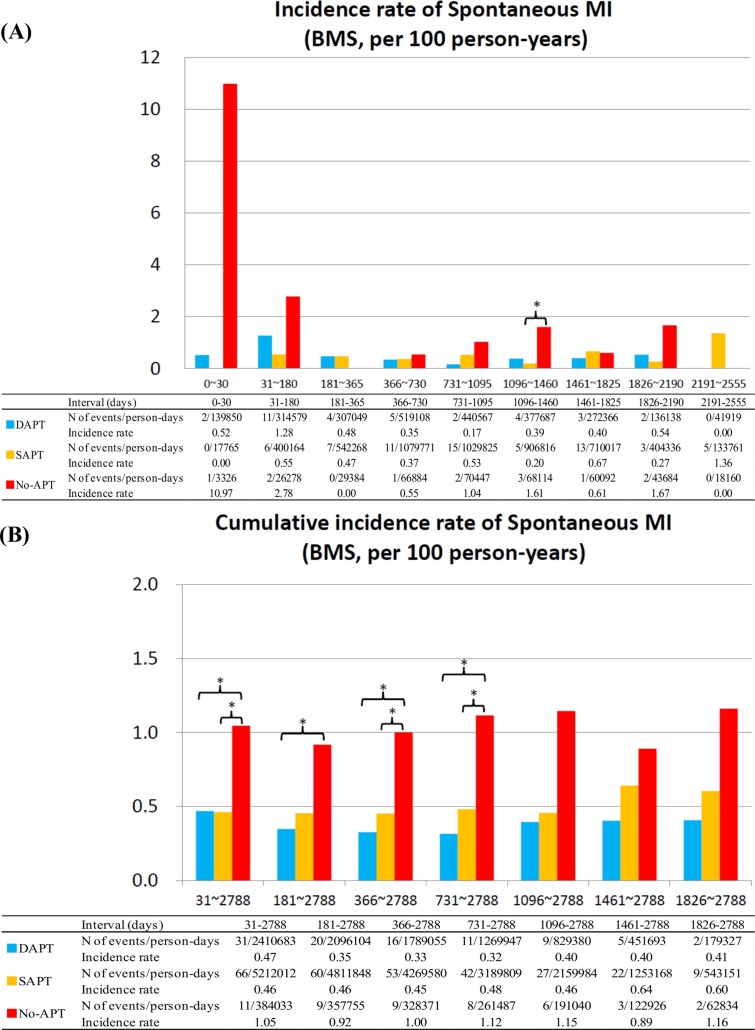
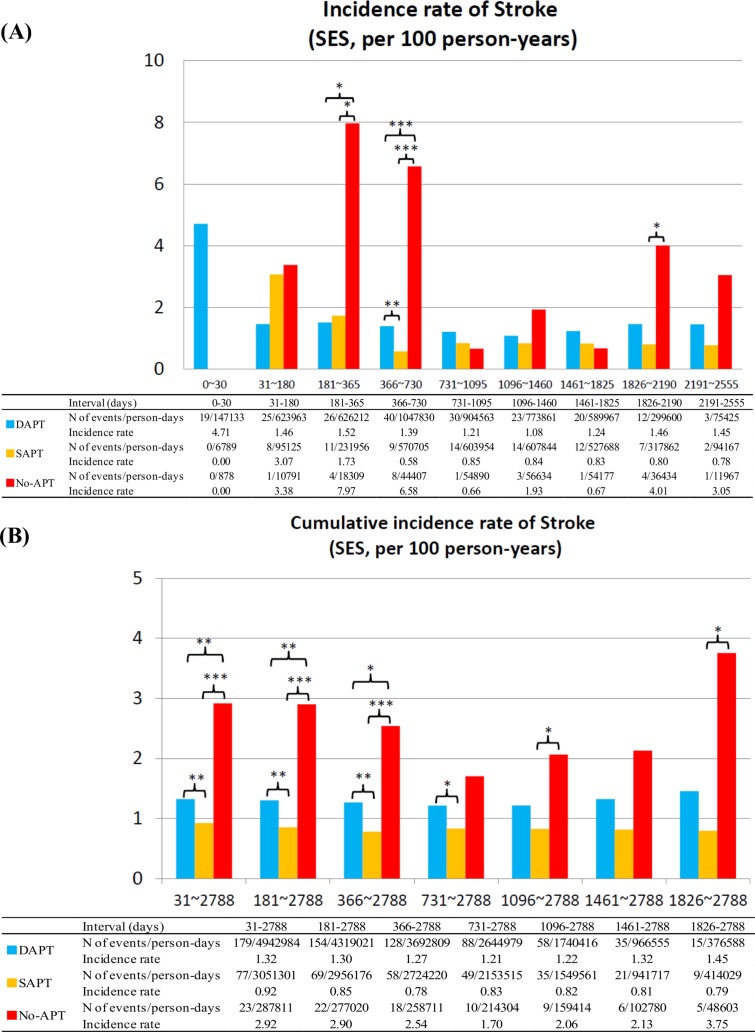
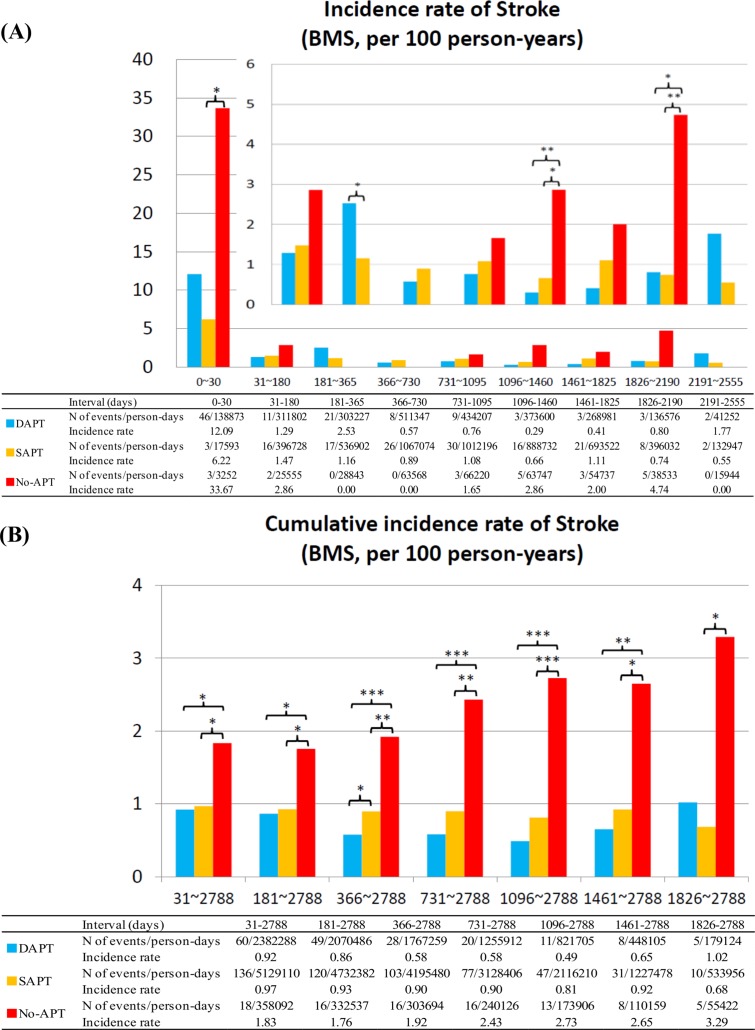
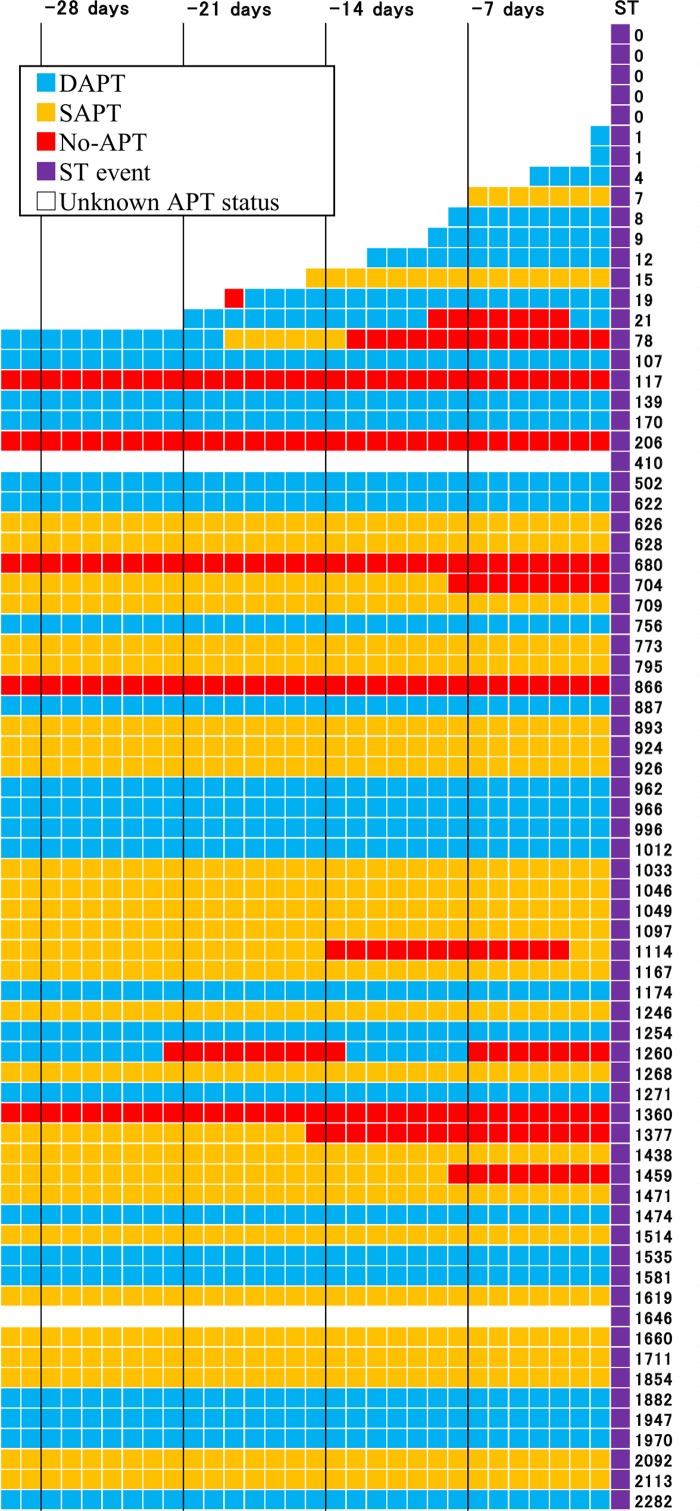
Relation of antiplatelet therapy (APT) discontinuation with the risk of serious cardiovascular events has not been fully addressed yet. This study is aimed to evaluate the risk of ischemic event after APT discontinuation based on long-term APT status of large cohort. In the CREDO-Kyoto Registry Cohort-2 enrolling 15939 consecutive patients undergoing first coronary revascularization, 10470 patients underwent percutaneous coronary intervention either with bare-metal stents (BMS) only (N=5392) or sirolimus-eluting stents (SES) only (N=5078). Proportions of patients taking dual-APT were 67.3% versus 33.4% at 1-year, and 48.7% versus 24.3% at 5-year in the SES and BMS strata, respectively. We evaluated daily APT status (dual-, single- and no-APT) and linked the adverse events to the APT status just 1-day before the events. No-APT as compared with dual- or single-APT was associated with significantly higher risk for stent thrombosis (ST) beyond 1-month after SES implantation (cumulative incidence rates beyond 1-month: 1.23 versus 0.15/0.29, P<0.001/P<0.001), while higher risk of no-APT for ST was evident only until 6-month after BMS implantation (incidence rates between 1- and 6-month: 8.43 versus 0.71/1.20, P<0.001/P<0.001, and cumulative incidence rates beyond 6-month: 0.31 versus 0.11/0.08, P=0.16/P=0.08). No-APT as compared with dual- or single-APT was also associated with significantly higher risk for spontaneous myocardial infarction (MI) and stroke regardless of the types of stents implanted. Single-APT as compared with dual-APT was not associated with higher risk for serious adverse events, except for the marginally higher risk for ST in the SES stratum. In conclusion, discontinuation of both aspirin and thienopyridines was associated with increased risk for serious cardiovascular events including ST, spontaneous MI and stroke beyond 1-month after coronary stenting.
Conflict of interest statement
Figures
Similar articles
-
Late adverse events after implantation of sirolimus-eluting stent and bare-metal stent: long-term (5-7 years) follow-up of the Coronary Revascularization Demonstrating Outcome study-Kyoto registry Cohort-2.Circ Cardiovasc Interv. 2014 Apr;7(2):168-79. doi: 10.1161/CIRCINTERVENTIONS.113.000987. Epub 2014 Feb 18. Circ Cardiovasc Interv. 2014. PMID: 24550439
-
Incidence and outcome of surgical procedures after coronary bare-metal and drug-eluting stent implantation: a report from the CREDO-Kyoto PCI/CABG registry cohort-2.Circ Cardiovasc Interv. 2012 Apr;5(2):237-46. doi: 10.1161/CIRCINTERVENTIONS.111.963728. Epub 2012 Mar 6. Circ Cardiovasc Interv. 2012. PMID: 22396582
-
Two-year outcomes after first- or second-generation drug-eluting or bare-metal stent implantation in all-comer patients undergoing percutaneous coronary intervention: a pre-specified analysis from the PRODIGY study (PROlonging Dual Antiplatelet Treatment After Grading stent-induced Intimal hyperplasia studY).JACC Cardiovasc Interv. 2014 Jan;7(1):20-8. doi: 10.1016/j.jcin.2013.09.008. Epub 2013 Dec 11. JACC Cardiovasc Interv. 2014. PMID: 24332420 Clinical Trial.
-
Stents and antiplatelet therapy.Adv Cardiol. 2012;47:114-24. doi: 10.1159/000338054. Epub 2012 Aug 9. Adv Cardiol. 2012. PMID: 22906907 Review.
-
Stent thrombosis and drug-eluting stents.J Cardiol. 2011 Sep;58(2):92-8. doi: 10.1016/j.jjcc.2011.07.003. Epub 2011 Aug 11. J Cardiol. 2011. PMID: 21839615 Review.
Cited by
-
Impact of Antiplatelet Therapies on Patients Outcome in Osteosynthetic Surgery of Proximal Femoral Fractures.J Clin Med. 2019 Dec 9;8(12):2176. doi: 10.3390/jcm8122176. J Clin Med. 2019. PMID: 31835361 Free PMC article.
-
Modifying the Interagency Emergency Health Kit to include treatment for non-communicable diseases in natural disasters and complex emergencies.BMJ Glob Health. 2016 Oct 20;1(3):e000128. doi: 10.1136/bmjgh-2016-000128. eCollection 2016. BMJ Glob Health. 2016. PMID: 28588970 Free PMC article.
-
Effects of Antithrombotic Treatment on Bleeding Complications of EBUS-TBNA.Medicina (Kaunas). 2021 Feb 5;57(2):142. doi: 10.3390/medicina57020142. Medicina (Kaunas). 2021. PMID: 33562541 Free PMC article.
-
Patterns of antiplatelet drug use after a first myocardial infarction during a 10-year period.Br J Clin Pharmacol. 2017 Mar;83(3):632-641. doi: 10.1111/bcp.13139. Epub 2016 Oct 24. Br J Clin Pharmacol. 2017. PMID: 27662521 Free PMC article.
References
-
- Iakovou I, Schmidt T, Bonizzoni E, Ge L, Sangiorgi GM, Stankovic G, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA. 2005;293: 2126–2130. - PubMed
-
- Eisenstein EL, Anstrom KJ, Kong DF, Shaw LK, Tuttle RH, Mark DB, et al. Clopidogrel use and long-term clinical outcomes after drug-eluting stent implantation. JAMA. 2007;297: 159–168. - PubMed
-
- Park DW, Park SW, Park KH, Lee BK, Kim YH, Lee CW, et al. Frequency of and risk factors for stent thrombosis after drug-eluting stent implantation during long-term follow-up. Am J Cardiol. 2006;98: 352–356. - PubMed
-
- Ho PM, Fihn SD, Wang L, Bryson CL, Lowy E, Maynard C, et al. Clopidogrel and long-term outcomes after stent implantation for acute coronary syndrome. Am Heart J. 2007;154: 846–851. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
