

Is the increased risk of preterm birth following excision for cervical intraepithelial neoplasia restricted to the first birth post treatment?
- PMID: 25854594
- PMCID: PMC5008142
- DOI: 10.1111/1471-0528.13398
Is the increased risk of preterm birth following excision for cervical intraepithelial neoplasia restricted to the first birth post treatment?
Abstract
Objective: To explore whether the increased risk of preterm birth following treatment for cervical disease is limited to the first birth following colposcopy.
Design: Nested case-control study.
Setting: Twelve NHS hospitals in England.
Population: All nonmultiple births from women selected as cases or controls from a cohort of women with both colposcopy and a hospital birth. Cases had a preterm (20-36 weeks of gestation) birth. Controls had a term birth (38-42 weeks) and no preterm.
Methods: Obstetric, colposcopy and pathology details were obtained.
Main outcome measures: Adjusted odds ratio of preterm birth in first and second or subsequent births following treatment for cervical disease.
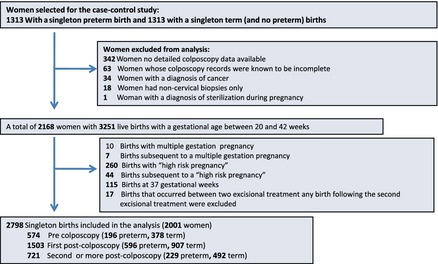
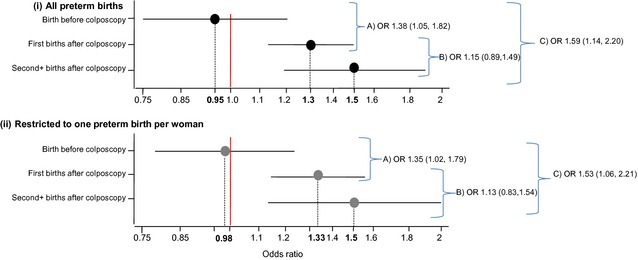
Results: A total of 2798 births (1021 preterm) from 2001 women were included in the analysis. The risk of preterm birth increased with increasing depth of treatment among first births post treatment [trend per category increase in depth, categories <10 mm, 10-14 mm, 15-19 mm, ≥20 mm: odds ratio (OR) 1.23, 95% confidence interval (95% CI) 1.12-1.36, P < 0.001] and among second and subsequent births post treatment (trend OR 1.34, 95% CI 1.15-1.56, P < 0.001). No trend was observed among births before colposcopy (OR 0.98, 95% CI 0.83-1.16, P = 0.855). The absolute risk of a preterm birth following deep treatments (≥15 mm) was 6.5% among births before colposcopy, 18.9% among first births and 17.2% among second and subsequent births post treatment. Risk of preterm birth (once depth was accounted for) did not differ when comparing first births post colposcopy with second and subsequent births post colposcopy (adjusted OR 1.15, 95% CI 0.89-1.49).
Conclusions: The increased risk of preterm birth following treatment for cervical disease is not restricted to the first birth post colposcopy; it remains for second and subsequent births. These results suggest that once a woman has a deep treatment she remains at higher risk of a preterm birth throughout her reproductive life.
Keywords: Cervical intraepithelial neoplasia; conisation; large loop excision of the transformation zone; preterm delivery.
© 2015 The Authors. BJOG An International Journal of Obstetrics and Gynaecology published by John Wiley & Sons Ltd on behalf of Royal College of Obstetricians and Gynaecologists.
Figures
References
-
- Bruinsma FJ, Quinn MA. The risk of preterm birth following treatment for precancerous changes in the cervix: a systematic review and meta‐analysis. BJOG 2011;118:1031–41. - PubMed
-
- Kyrgiou M, Koliopoulos G, Martin‐Hirsch PL, Arbyn M, Prendiville W, Paraskevaidis E. Obstetric outcome after conservative treatment for intraepithelial or early invasive cervical lesions: systematic review and meta‐analysis. Lancet 2006;367:489–98. - PubMed
-
- Sadler L, Saftlas A, Wang W, Exeter M, Whittaker J, McCowan L. Treatment for cervical intraepithelial neoplasia and risk of preterm delivery. JAMA 2004;291:2100–6. - PubMed
-
- Noehr B, Jensen A, Frederiksen K, Tabor A, Kjaer SK. Depth of cervical cone removed by loop electrosurgical excision procedure and subsequent risk of spontaneous preterm delivery. Obstet Gynecol 2009;114:1232–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
