

β-blocker use and mortality in COPD patients after myocardial infarction: a Swedish nationwide observational study
- PMID: 25854796
- PMCID: PMC4579937
- DOI: 10.1161/JAHA.114.001611
β-blocker use and mortality in COPD patients after myocardial infarction: a Swedish nationwide observational study
Abstract
Background: Patients with myocardial infarction (MI) and concomitant chronic obstructive pulmonary disease (COPD) constitute a high-risk group with increased mortality. β-Blocker therapy has been shown to reduce mortality, prevent arrhythmias, and delay heart failure development after an MI in broad populations. However, the effect of β-blockers in COPD patients is less well established and they may also be less treated due to fear of adverse reactions. We investigated β-blocker prescription at discharge in patients with COPD after MI.
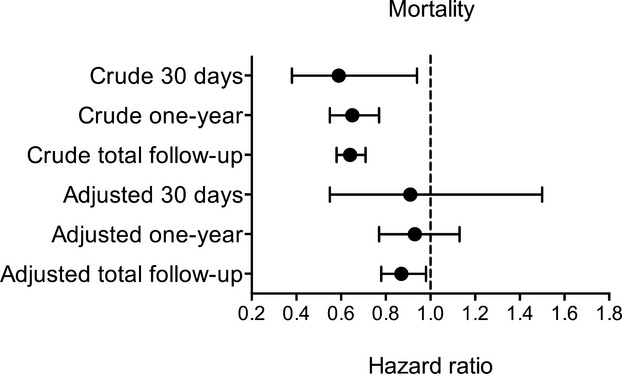
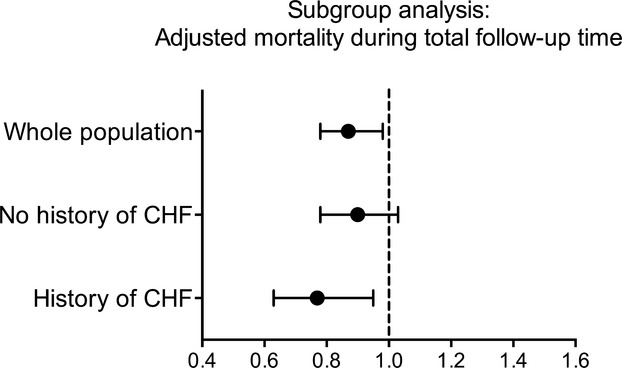
Methods and results: Patients hospitalized for MI between 2005 and 2010 were identified from the nationwide Swedish SWEDEHEART registry. Patients with COPD who were alive and discharged after an MI were selected as the study population. In this cohort, patients who were discharged with β-blockers were compared to patients not discharged with β-blockers. The primary end point was all-cause mortality. A total of 4858 patients were included, of which 4086 (84.1%) were discharged with a β-blocker while 772 (15.9%) were not. After adjusting for potential confounders including baseline characteristics, comorbidities, and in-hospital characteristics, patients discharged with a β-blocker had lower all-cause mortality (hazard ratio 0.87, 95% CI 0.78 to 0.98) during the total follow-up time (maximum 7.2 years). In the subgroup of patients with a history of heart failure, the corresponding hazard ratio was 0.77 (95% CI 0.63 to 0.95).
Conclusions: Patients with COPD discharged with β-blockers after an MI had a lower all-cause mortality compared to patients not prescribed β-blockers. The results indicate that MI patients with COPD may benefit from β-blockers.
Keywords: epidemiology; mortality; myocardial infarction; prevention.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Task Force on the management of ST‐segment elevation acute myocardial infarction of the European Society of Cardiology (ESC). Steg PG, James SK, Atar D, Badano LP, Blomstrom‐Lundqvist C, Borger MA, Di MC, Dickstein K, Ducrocq G, Fernandez‐Aviles F, Gershlick AH, Giannuzzi P, Halvorsen S, Huber K, Juni P, Kastrati A, Knuuti J, Lenzen MJ, Mahaffey KW, Valgimigli M, van‘t Hof A, Widimsky P, Zahger D. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST‐segment elevation. Eur Heart J. 2012; 33:2569-2619. - PubMed
-
- Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, Bueno H, Caso P, Dudek D, Gielen S, Huber K, Ohman M, Petrie MC, Sonntag F, Uva MS, Storey RF, Wijns W, Zahger DGuidelines ESCCfP. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST‐segment elevation: The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST‐segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2011; 32:2999-3054. - PubMed
-
- Group TNMS. Timolol‐induced reduction in mortality and reinfarction in patients surviving acute myocardial infarction. N Engl J Med. 1981; 304:801-807. - PubMed
-
- Hjalmarson A, Herlitz J, Holmberg S, Ryden L, Swedberg K, Vedin A, Waagstein F, Waldenstrom A, Waldenstrom J, Wedel H, Wilhelmsen L, Wilhelmsson C. The Goteborg metoprolol trial. Effects on mortality and morbidity in acute myocardial infarction. Circulation. 1983; 67:I26-I32. - PubMed
-
- Gottlieb SS, McCarter RJ, Vogel RA. Effect of beta‐blockade on mortality among high‐risk and low‐risk patients after myocardial infarction. N Engl J Med. 1998; 339:489-497. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
