

The brain connectome as a personalized biomarker of seizure outcomes after temporal lobectomy
- PMID: 25854868
- PMCID: PMC4433467
- DOI: 10.1212/WNL.0000000000001548
The brain connectome as a personalized biomarker of seizure outcomes after temporal lobectomy
Abstract
Objective: We examined whether individual neuronal architecture obtained from the brain connectome can be used to estimate the surgical success of anterior temporal lobectomy (ATL) in patients with temporal lobe epilepsy (TLE).
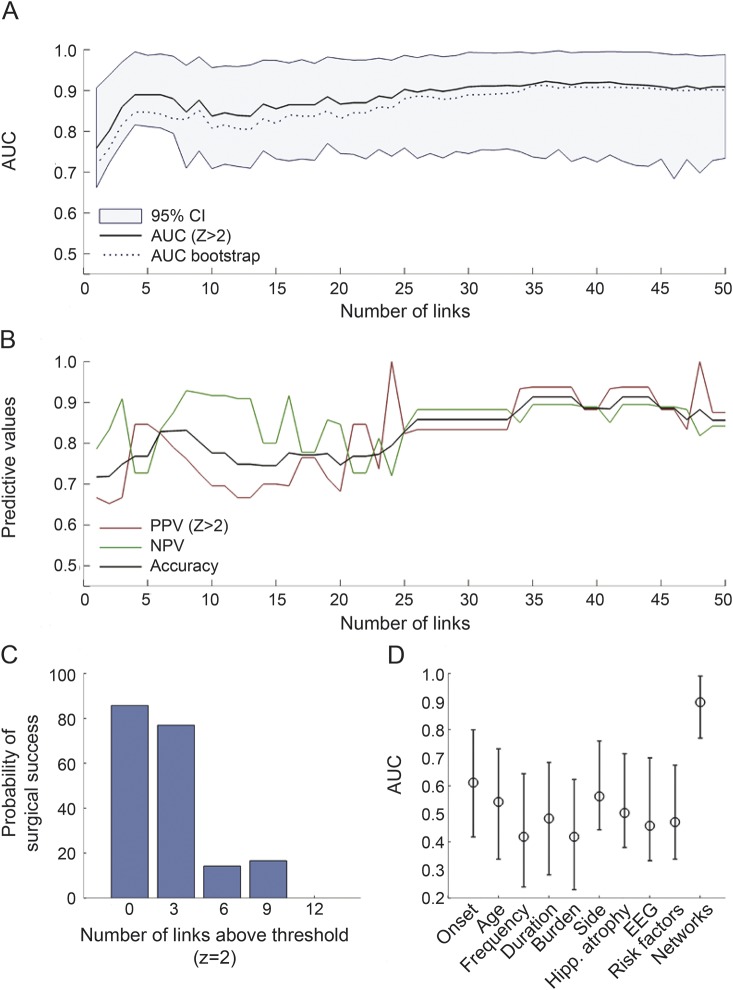
Methods: We retrospectively studied 35 consecutive patients with TLE who underwent ATL. The structural brain connectome was reconstructed from all patients using presurgical diffusion MRI. Network links in patients were standardized as Z scores based on connectomes reconstructed from healthy controls. The topography of abnormalities in linkwise elements of the connectome was assessed on subnetworks linking ipsilateral temporal with extratemporal regions. Predictive models were constructed based on the individual prevalence of linkwise Z scores >2 and based on presurgical clinical data.
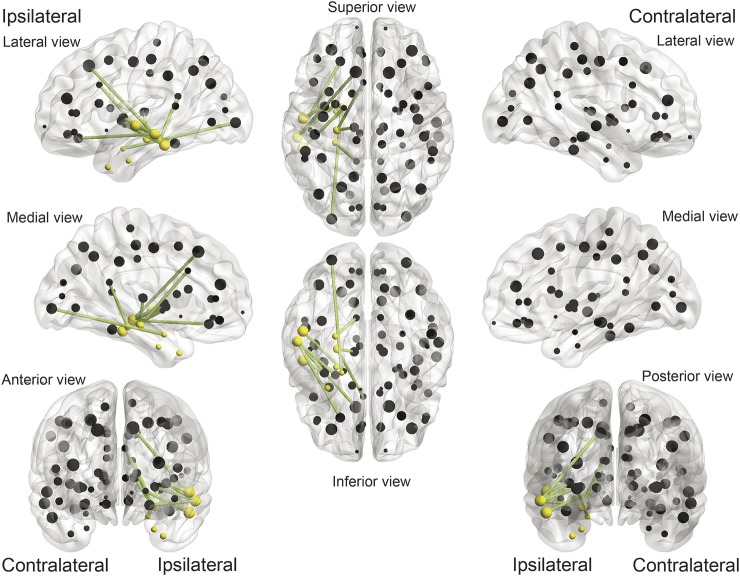
Results: Patients were more likely to achieve postsurgical seizure freedom if they exhibited fewer abnormalities within a subnetwork composed of the ipsilateral hippocampus, amygdala, thalamus, superior frontal region, lateral temporal gyri, insula, orbitofrontal cortex, cingulate, and lateral occipital gyrus. Seizure-free surgical outcome was predicted by neural architecture alone with 90% specificity (83% accuracy), and by neural architecture combined with clinical data with 94% specificity (88% accuracy).
Conclusions: Individual variations in connectome topography, combined with presurgical clinical data, may be used as biomarkers to better estimate surgical outcomes in patients with TLE.
© 2015 American Academy of Neurology.
Figures

References
-
- Margerison JH, Corsellis JA. Epilepsy and the temporal lobes: a clinical, electroencephalographic and neuropathological study of the brain in epilepsy, with particular reference to the temporal lobes. Brain 1966;89:499–530. - PubMed
-
- Wiebe S. Epidemiology of temporal lobe epilepsy. Can J Neurol Sci 2000;27(suppl 1):S6–S10; discussion S20–S21. - PubMed
-
- Cahan LD, Engel J., Jr Surgery for epilepsy: a review. Acta Neurol Scand 1986;73:551–560. - PubMed
-
- Wiebe S, Blume WT, Girvin JP, Eliasziw M. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med 2001;345:311–318. - PubMed
-
- Tellez-Zenteno JF, Wiebe S. Long-term seizure and psychosocial outcomes of epilepsy surgery. Curr Treat Options Neurol 2008;10:253–259. - PubMed