

Impact of Male and Female Weight, Smoking, and Intercourse Frequency on Live Birth in Women With Polycystic Ovary Syndrome
- PMID: 25856211
- PMCID: PMC4454812
- DOI: 10.1210/jc.2015-1178
Impact of Male and Female Weight, Smoking, and Intercourse Frequency on Live Birth in Women With Polycystic Ovary Syndrome
Abstract
Context: Obese men with normal semen parameters exhibit reduced fertility but few prospective data are available.
Objective: This study aimed to determine the effect of male factors and body mass among the Pregnancy in Polycystic Ovary Syndrome II (PPCOS II) participants.
Methods: This is a secondary analysis of the PPCOS II trial. A total of 750 infertile women with polycystic ovary syndrome (PCOS) were randomly assigned to up to receive five cycles of letrozole or clomiphene citrate. Females were 18-39-years-old and had a male partner with sperm concentration of at least 14 million/mL who consented to regular intercourse. Analysis was limited to couples with complete male partner information (n = 710).
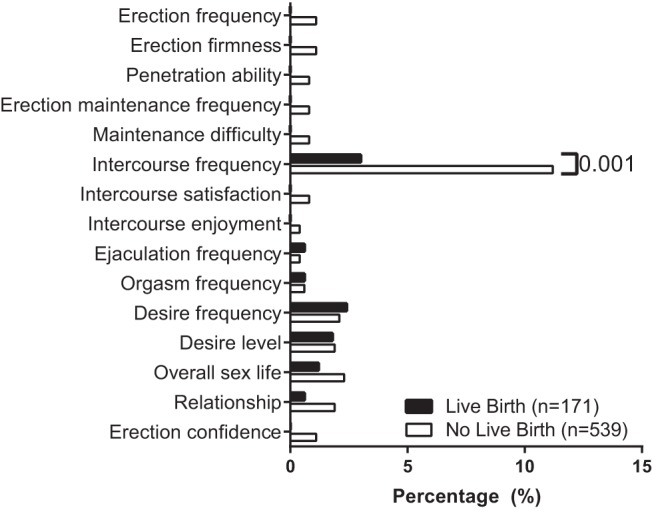
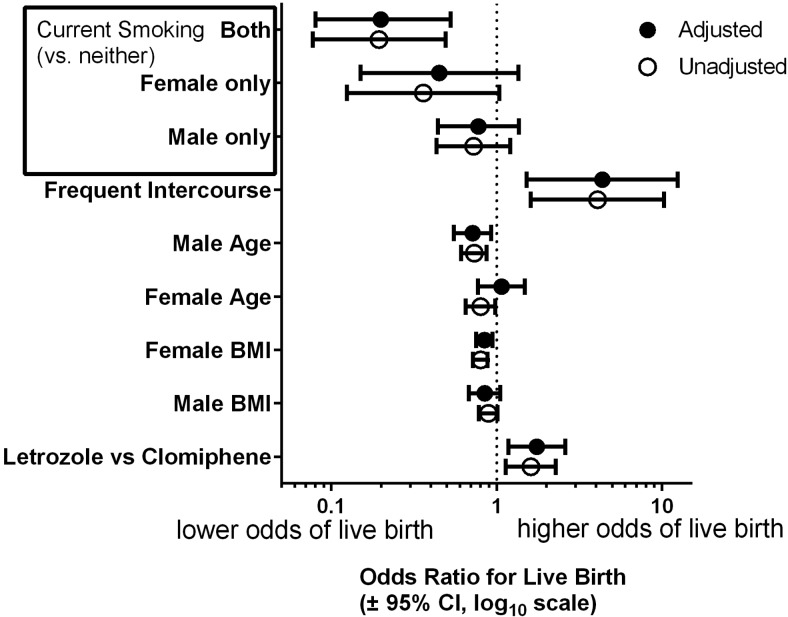
Results: Male body mass index (BMI) was higher in couples who failed to conceive (29.5 kg/m(2) vs 28.2 kg/m(2); P = .039) as well as those who did not achieve a live birth (29.5 kg/m(2) vs 28.1 kg/m(2); P = .047). At least one partner was obese in 548 couples (77.1%). A total of 261 couples were concordant for obesity (36.8%). After adjustment for female BMI, the association of male BMI with live birth was no longer significant (odds ratio [OR] = 0.85; 95 % confidence interval [CI], 0.68-1.05; P = .13). Couples in which both partners smoked had a lower chance of live birth vs nonsmokers (OR = 0.20; 95 % CI, 0.08-0.52; P = .02), whereas there was not a significant effect of female or male smoking alone. Live birth was more likely in couples with at least three sexual intercourse attempts over the previous 4 weeks (reported at baseline) as opposed to couples with lesser frequency (OR = 4.39; 95 % CI, 1.52-12. 4; P < .01).
Conclusions: In this large cohort of obese women with PCOS, effect of male obesity was explained by female BMI. Lower chance of success was seen among couples where both partners smoked. Obesity and smoking are common among women with PCOS and their partners and contribute to a decrease in fertility treatment success.
Figures
Similar articles
-
Metabolic syndrome in obesity: treatment success and adverse pregnancy outcomes with ovulation induction in polycystic ovary syndrome.Am J Obstet Gynecol. 2021 Sep;225(3):280.e1-280.e11. doi: 10.1016/j.ajog.2021.03.048. Epub 2021 Apr 20. Am J Obstet Gynecol. 2021. PMID: 33852887 Free PMC article. Clinical Trial.
-
Letrozole versus clomiphene for infertility in the polycystic ovary syndrome.N Engl J Med. 2014 Jul 10;371(2):119-29. doi: 10.1056/NEJMoa1313517. N Engl J Med. 2014. PMID: 25006718 Free PMC article. Clinical Trial.
-
The Pregnancy in Polycystic Ovary Syndrome II (PPCOS II) trial: rationale and design of a double-blind randomized trial of clomiphene citrate and letrozole for the treatment of infertility in women with polycystic ovary syndrome.Contemp Clin Trials. 2012 May;33(3):470-81. doi: 10.1016/j.cct.2011.12.005. Epub 2012 Jan 13. Contemp Clin Trials. 2012. PMID: 22265923 Free PMC article. Clinical Trial.
-
Endocrine and reproductive effects of polycystic ovarian syndrome.Obstet Gynecol Clin North Am. 2015 Mar;42(1):55-65. doi: 10.1016/j.ogc.2014.09.003. Epub 2014 Dec 13. Obstet Gynecol Clin North Am. 2015. PMID: 25681840 Review.
-
Intra-uterine insemination for unexplained subfertility.Cochrane Database Syst Rev. 2020 Mar 3;3(3):CD001838. doi: 10.1002/14651858.CD001838.pub6. Cochrane Database Syst Rev. 2020. PMID: 32124980 Free PMC article.
Cited by
-
Metabolic Concomitants of Obese and Nonobese Women With Features of Polycystic Ovarian Syndrome.J Endocr Soc. 2017 Nov 2;1(12):1417-1427. doi: 10.1210/js.2017-00323. eCollection 2017 Dec 1. J Endocr Soc. 2017. PMID: 29264465 Free PMC article.
-
Suitability of the National Health Care Surveys to Examine Behavioral Health Services Associated with Polycystic Ovary Syndrome.J Behav Health Serv Res. 2018 Apr;45(2):252-268. doi: 10.1007/s11414-016-9543-6. J Behav Health Serv Res. 2018. PMID: 27966057 Free PMC article.
-
Comparison of sonohysterography to hysterosalpingogram for tubal patency assessment in a multicenter fertility treatment trial among women with polycystic ovary syndrome.J Assist Reprod Genet. 2018 Dec;35(12):2173-2180. doi: 10.1007/s10815-018-1306-2. Epub 2018 Sep 7. J Assist Reprod Genet. 2018. PMID: 30194618 Free PMC article.
References
-
- Lake JK, Power C, Cole TJ. Women's reproductive health: The role of body mass index in early and adult life. Int J Obes Relat Metab Disord. 1997;21:432–438. - PubMed
-
- Metwally M, Saravelos SH, Ledger WL, Li TC. Body mass index and risk of miscarriage in women with recurrent miscarriage. Fertil Steril. 2010;94:290–295. - PubMed
-
- Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systematic review and meta-analysis. JAMA. 2009;301:636–650. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 HD039005/HD/NICHD NIH HHS/United States
- U10 HD33172/HD/NICHD NIH HHS/United States
- U10 HD055936/HD/NICHD NIH HHS/United States
- U10 HD055925/HD/NICHD NIH HHS/United States
- U10 HD38998/HD/NICHD NIH HHS/United States
- U10 HD038998/HD/NICHD NIH HHS/United States
- U10-HD27049/HD/NICHD NIH HHS/United States
- U10 HD055944/HD/NICHD NIH HHS/United States
- U10 HD39005/HD/NICHD NIH HHS/United States
- U10 HD038992/HD/NICHD NIH HHS/United States
- U54-HD29834/HD/NICHD NIH HHS/United States
- U10 HD38992/HD/NICHD NIH HHS/United States
- U10HD055925/HD/NICHD NIH HHS/United States
- U10 HD033172/HD/NICHD NIH HHS/United States
- R01 HD029834/HD/NICHD NIH HHS/United States
- U10 HD027049/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
