

Effectiveness of community-based integrated care in frail COPD patients: a randomised controlled trial
- PMID: 25856791
- PMCID: PMC4532156
- DOI: 10.1038/npjpcrm.2015.22
Effectiveness of community-based integrated care in frail COPD patients: a randomised controlled trial
Abstract
Background: Chronic obstructive pulmonary disease (COPD) generates a high burden on health care, and hospital admissions represent a substantial proportion of the overall costs of the disease. Integrated care (IC) has shown efficacy to reduce hospitalisations in COPD patients at a pilot level. Deployment strategies for IC services require assessment of effectiveness at the health care system level.
Aims: The aim of this study was to explore the effectiveness of a community-based IC service in preventing hospitalisations and emergency department (ED) visits in stable frail COPD patients.
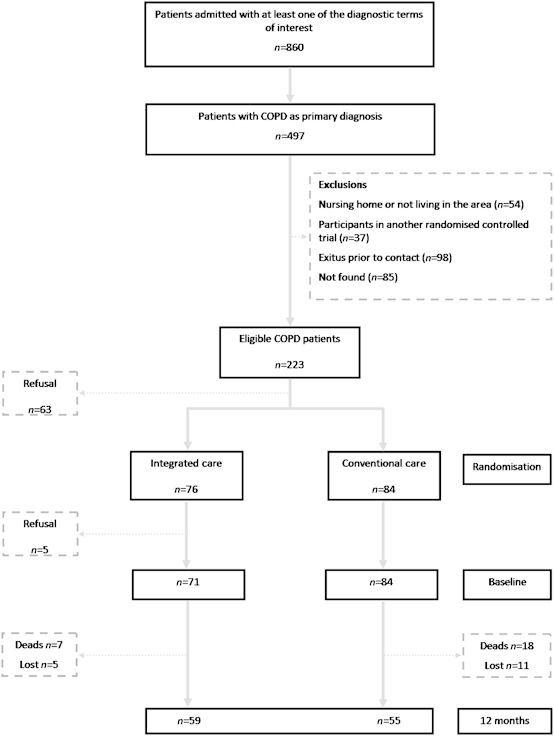
Methods: From April to December 2005, 155 frail community-dwelling COPD patients were randomly allocated either to IC (n=76, age 73 (8) years, forced expiratory volume during the first second, FEV1 41(19) % predicted) or usual care (n=84, age 75(9) years, FEV1 44 (20) % predicted) and followed up for 12 months. The IC intervention consisted of the following: (a) patient's empowerment for self-management; (b) an individualised care plan; (c) access to a call centre; and (d) coordination between the levels of care. Thereafter, hospital admissions, ED visits and mortality were monitored for 6 years.
Results: IC enhanced self-management (P=0.02), reduced anxiety-depression (P=0.001) and improved health-related quality of life (P=0.02). IC reduced both ED visits (P=0.02) and mortality (P=0.03) but not hospital admission. No differences between the two groups were seen after 6 years.
Conclusion: The intervention improved clinical outcomes including survival and decreased the ED visits, but it did not reduce hospital admissions. The study facilitated the identification of two key requirements for adoption of IC services in the community: appropriate risk stratification of patients, and preparation of the community-based work force.
References
-
- Lopez-Campos JL, Hartl S, Pozo-Rodriguez F, Roberts CM. Variability of hospital resources for acute care of COPD patients: European COPD Audit. Eur Respir J. 2013;43:754–762. - PubMed
-
- World Health Organization Chronic obstructive pulmonary disease (COPD) 2014 ). http://www.who.int/respiratory/copd/en/ , accessed on 20 September 2014.
-
- Murray CJ, Lopez AD. Measuring the global burden of disease. N Engl J Med. 2013;369:448–457. - PubMed
-
- Sullivan SD, Ramsey SD, Lee TA. The economic burden of COPD. Chest. 2000;117:5S–9S. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
