

High Local Concentrations of Intradermal MSCs Restore Skin Integrity and Facilitate Wound Healing in Dystrophic Epidermolysis Bullosa
- PMID: 25858020
- PMCID: PMC4817872
- DOI: 10.1038/mt.2015.58
High Local Concentrations of Intradermal MSCs Restore Skin Integrity and Facilitate Wound Healing in Dystrophic Epidermolysis Bullosa
Abstract
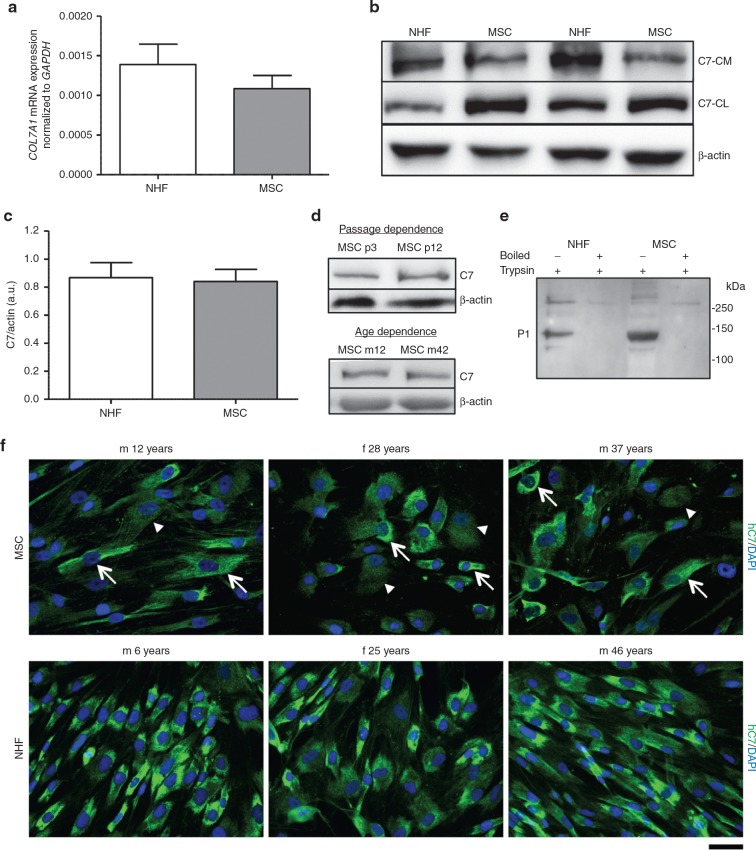
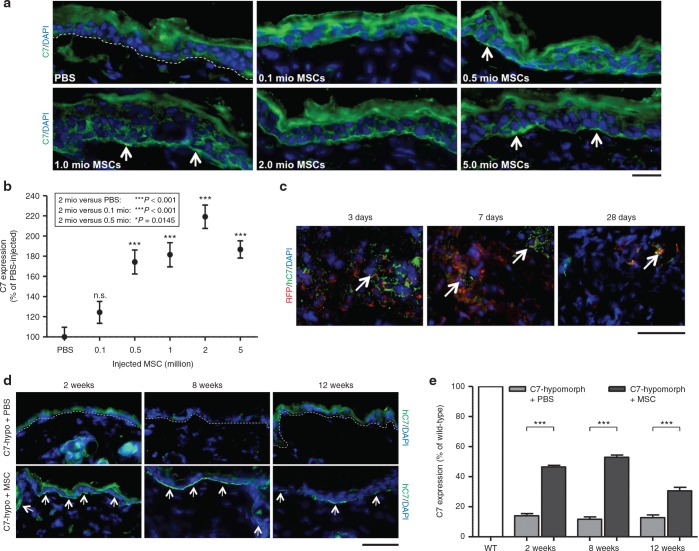
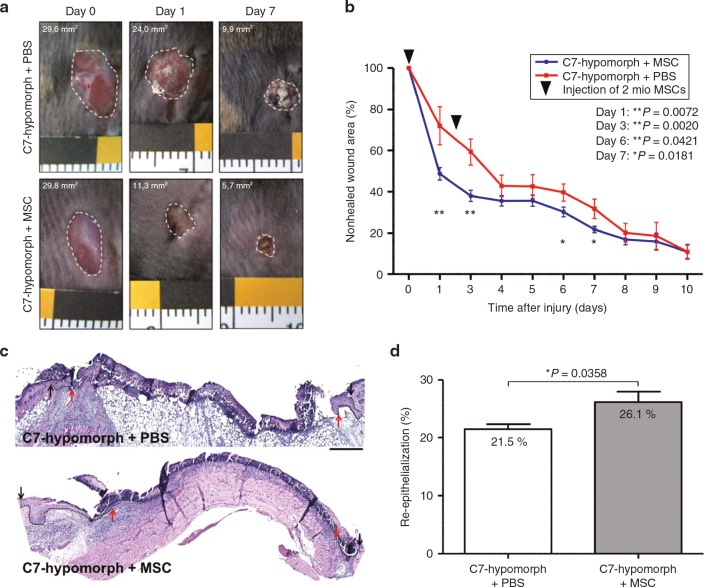
Dystrophic epidermolysis bullosa (DEB) is an incurable skin fragility disorder caused by mutations in the COL7A1 gene, coding for the anchoring fibril protein collagen VII (C7). Life-long mechanosensitivity of skin and mucosal surfaces is associated with large body surface erosions, chronic wounds, and secondary fibrosis that severely impede functionality. Here, we present the first systematic long-term evaluation of the therapeutic potential of a mesenchymal stromal cell (MSC)-based therapy for DEB. Intradermal administration of MSCs in a DEB mouse model resulted in production and deposition of C7 at the dermal-epidermal junction, the physiological site of function. The effect was dose-dependent with MSCs being up to 10-fold more potent than dermal fibroblasts. MSCs promoted regeneration of DEB wounds via normalization of dermal and epidermal healing and improved skin integrity through de novo formation of functional immature anchoring fibrils. Additional benefits were gained by MSCs' anti-inflammatory effects, which led to decreased immune cell infiltration into injured DEB skin. In our setting, the clinical benefit of MSC injections lasted for more than 3 months. We conclude that MSCs are viable options for localized DEB therapy. Importantly, however, the cell number needed to achieve therapeutic efficacy excludes the use of systemic administration.
Figures


Comment in
-
From Mesoderm to Mesodermatology: Bone Marrow Mesenchymal Cells Heal Skin Wounds.Mol Ther. 2015 Aug;23(8):1283-1284. doi: 10.1038/mt.2015.84. Mol Ther. 2015. PMID: 26227251 Free PMC article. No abstract available.
References
-
- Aymé, S, Rodwell, C, eds. (2013). 2013 Report on the State of the Art of Rare Disease Activities in Europe. Publisher: European Union, Brussels.
-
- Fine, JD, Bruckner-Tuderman, L, Eady, RA, Bauer, EA, Bauer, JW, Has, C et al. (2014). Inherited epidermolysis bullosa: updated recommendations on diagnosis and classification. J Am Acad Dermatol 70: 1103–1126. - PubMed
-
- Has, C and Bruckner-Tuderman, L (2014). The genetics of skin fragility. Annu Rev Genomics Hum Genet 15: 245–268. - PubMed
-
- Van Agtmael, T and Bruckner-Tuderman, L (2010). Basement membranes and human disease. Cell Tissue Res 339: 167–188. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
