

Robotic Level III Inferior Vena Cava Tumor Thrombectomy: Initial Series
- PMID: 25858419
- PMCID: PMC9083507
- DOI: 10.1016/j.juro.2015.03.119
Robotic Level III Inferior Vena Cava Tumor Thrombectomy: Initial Series
Abstract
Purpose: Level III inferior vena cava tumor thrombectomy for renal cancer is one of the most challenging open urologic oncology surgeries. We present the initial series of completely intracorporeal robotic level III inferior vena cava tumor thrombectomy.
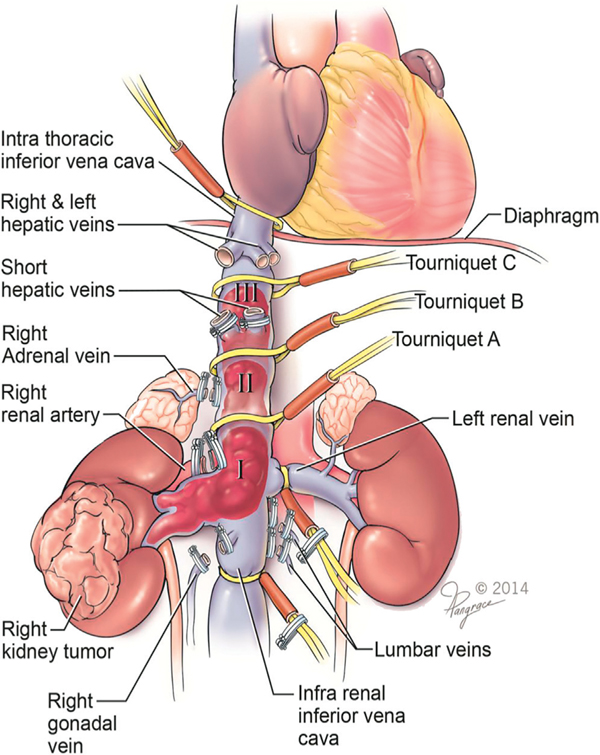
Materials and methods: Nine patients underwent robotic level III inferior vena cava thrombectomy and 7 patients underwent level II thrombectomy. The entire operation (high intrahepatic inferior vena cava control, caval exclusion, tumor thrombectomy, inferior vena cava repair, radical nephrectomy, retroperitoneal lymphadenectomy) was performed exclusively robotically. To minimize the chances of intraoperative inferior vena cava thrombus embolization, an "inferior vena cava-first, kidney-last" robotic technique was developed. Data were accrued prospectively.
Results: All 16 robotic procedures were successful, without open conversion or mortality. For level III cases (9), median primary kidney (right 6, left 3) cancer size was 8.5 cm (range 5.3 to 10.8) and inferior vena cava thrombus length was 5.7 cm (range 4 to 7). Median operative time was 4.9 hours (range 4.5 to 6.3), estimated blood loss was 375 cc (range 200 to 7,000) and hospital stay was 4.5 days. All surgical margins were negative. There were no intraoperative complications and 1 postoperative complication (Clavien 3b). At a median 7 months of followup (range 1 to 18) all patients are alive. Compared to level II thrombi the level III cohort trended toward greater inferior vena cava thrombus length (3.3 vs 5.7 cm), operative time (4.5 vs 4.9 hours) and blood loss (290 vs 375 cc).
Conclusions: With appropriate patient selection, surgical planning and robotic experience, completely intracorporeal robotic level III inferior vena cava thrombectomy is feasible and can be performed efficiently. Larger experience, longer followup and comparison with open surgery are needed to confirm these initial outcomes.
Keywords: inferior; robotics; thrombectomy; vena cava.
Copyright © 2015 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Editorial Comment.J Urol. 2015 Oct;194(4):937; discussion 937-8. doi: 10.1016/j.juro.2015.03.138. Epub 2015 Jul 17. J Urol. 2015. PMID: 26193057 No abstract available.
-
Re: Robotic Level III Inferior Vena Cava Tumor Thrombectomy: Initial Series: I. S. Gill, C. Metcalfe, A. Abreu, V. Duddalwar, S. Chopra, M. Cunningham, D. Thangathurai, O. Ukimura, R. Satkunasivam, A. Hung, R. Papalia, M. Aron, M. Desai and M. Gallucci J Urol 2015;194:929-938.J Urol. 2016 Aug;196(2):622-3. doi: 10.1016/j.juro.2016.02.2979. Epub 2016 May 6. J Urol. 2016. PMID: 27156908 No abstract available.
-
Urologic Oncologic SurveyRobotic level III inferior vena cava tumor thrombectomy: Initial series. Gill IS, Metcalfe C, Abreu A, Duddalwar V, Chopra S, Cunningham M, Thangathurai D, Ukimura O, Satkunasivam R, Hung A, Papalia R, Aron M, Desai M, Gallucci M. J Urol. 2015 Oct;194(4):929-938. [Epub 2015 Apr 6]. doi: 10.1016/j.juro.2015.03.119.Urol Oncol. 2017 May;35(5):311. doi: 10.1016/j.urolonc.2016.05.010. Epub 2017 Mar 23. Urol Oncol. 2017. PMID: 28342659
Similar articles
-
Urologic Oncologic SurveyRobotic level III inferior vena cava tumor thrombectomy: Initial series. Gill IS, Metcalfe C, Abreu A, Duddalwar V, Chopra S, Cunningham M, Thangathurai D, Ukimura O, Satkunasivam R, Hung A, Papalia R, Aron M, Desai M, Gallucci M. J Urol. 2015 Oct;194(4):929-938. [Epub 2015 Apr 6]. doi: 10.1016/j.juro.2015.03.119.Urol Oncol. 2017 May;35(5):311. doi: 10.1016/j.urolonc.2016.05.010. Epub 2017 Mar 23. Urol Oncol. 2017. PMID: 28342659
-
Robot-assisted Level II-III Inferior Vena Cava Tumor Thrombectomy: Step-by-Step Technique and 1-Year Outcomes.Eur Urol. 2017 Aug;72(2):267-274. doi: 10.1016/j.eururo.2016.08.066. Epub 2016 Sep 20. Eur Urol. 2017. PMID: 27663048 Free PMC article.
-
Multi-Institutional Experience with Robotic Nephrectomy with Inferior Vena Cava Tumor Thrombectomy.J Urol. 2016 Apr;195(4 Pt 1):865-71. doi: 10.1016/j.juro.2015.09.094. Epub 2015 Nov 19. J Urol. 2016. PMID: 26602891
-
Review of Robotic-Assisted Radical Nephrectomy with Inferior Vena Cava Thrombectomy in Renal Cell Carcinoma.Curr Urol Rep. 2022 Dec;23(12):363-370. doi: 10.1007/s11934-022-01120-x. Epub 2022 Dec 1. Curr Urol Rep. 2022. PMID: 36454370 Review.
-
Robot-assisted hepatic mobilization and control of suprahepatic infradiaphragmatic inferior vena cava for level 3 vena caval thrombectomy: An IDEAL stage 0 study.J Surg Oncol. 2015 Dec;112(7):741-5. doi: 10.1002/jso.23980. Epub 2015 Aug 11. J Surg Oncol. 2015. PMID: 26265131 Review.
Cited by
-
Robotic surgery with the Da Vinci Xi: simultaneous upper and lower tract surgery.J Robot Surg. 2017 Sep;11(3):373-374. doi: 10.1007/s11701-016-0610-z. Epub 2016 Jun 17. J Robot Surg. 2017. PMID: 27314859 Review.
-
Step-by-step and orderly lowering of the height of inferior vena cava tumor thrombus is the key to robot-assisted thrombectomy for Mayo III/IV tumor thrombus.BMC Cancer. 2022 Feb 7;22(1):151. doi: 10.1186/s12885-022-09235-7. BMC Cancer. 2022. PMID: 35130848 Free PMC article.
-
Surgical and Oncological Outcomes of Level III-IV Versus Level I-II Inferior Vena Cava Thrombectomy: A Decennial Experience of a High-Volume European Referral Center.Ann Surg Oncol. 2024 Nov;31(12):8383-8393. doi: 10.1245/s10434-024-15878-6. Epub 2024 Jul 26. Ann Surg Oncol. 2024. PMID: 39060696
-
Robot-assisted radical nephrectomy and inferior vena cava tumor thrombectomy: Initial experience in Japan.IJU Case Rep. 2022 Jan 25;5(3):145-148. doi: 10.1002/iju5.12419. eCollection 2022 May. IJU Case Rep. 2022. PMID: 35509774 Free PMC article.
-
Surgical treatment of kidney tumors - contemporary trends in clinical practice.Cent European J Urol. 2016;69(4):341-346. doi: 10.5173/ceju.2016.845. Epub 2016 Sep 22. Cent European J Urol. 2016. PMID: 28127448 Free PMC article.
References
-
- Blute ML, Leibovich BC, Lohse CM et al.: The Mayo Clinic experience with surgical management, complications and outcome for patients with renal cell carcinoma and venous tumour thrombus. BJU Int 2004; 94: 33. - PubMed
-
- Al Otaibi M, Abou Youssif T, Alkhaldi A et al.: Renal cell carcinoma with inferior vena caval extension: impact of tumour extent on surgical outcome. BJU Int 2009; 104: 1467. - PubMed
-
- Neves RJ and Zincke H: Surgical treatment of renal cancer with vena cava extension. Br J Urol 1987; 59: 390. - PubMed
-
- Fergany AF, Gill IS, Kaouk JH et al.: Laparoscopic radical nephrectomy with level II vena caval thrombectomy: survival porcine study. J Urol 2002; 168: 2629. - PubMed
-
- Meraney AM, Gill IS, Desai M et al.: Laparoscopic inferior vena cava and right atrial thrombectomy utilizing deep hypothermic circulatory arrest. J Endourol 2003; 17: 275. - PubMed
