

Individualizing risk of multidrug-resistant pathogens in community-onset pneumonia
- PMID: 25860142
- PMCID: PMC4393134
- DOI: 10.1371/journal.pone.0119528
Individualizing risk of multidrug-resistant pathogens in community-onset pneumonia
Abstract
Introduction: The diffusion of multidrug-resistant (MDR) bacteria has created the need to identify risk factors for acquiring resistant pathogens in patients living in the community.
Objective: To analyze clinical features of patients with community-onset pneumonia due to MDR pathogens, to evaluate performance of existing scoring tools and to develop a bedside risk score for an early identification of these patients in the Emergency Department.
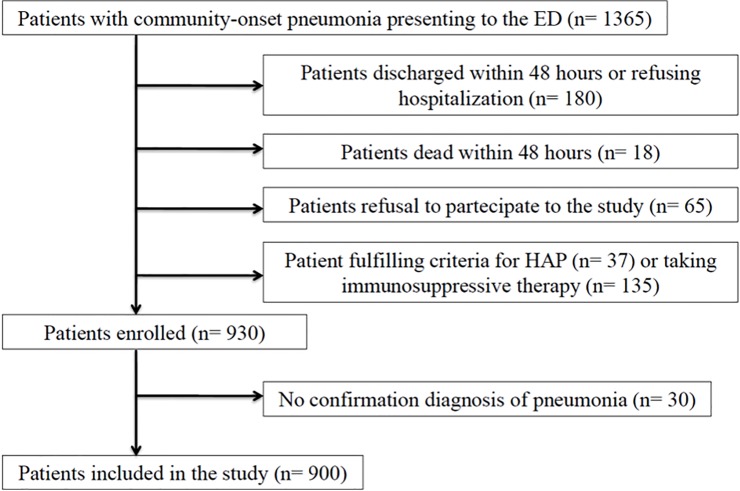
Patients and methods: This was an open, observational, prospective study of consecutive patients with pneumonia, coming from the community, from January 2011 to January 2013. The new score was validated on an external cohort of 929 patients with pneumonia admitted in internal medicine departments participating at a multicenter prospective study in Spain.
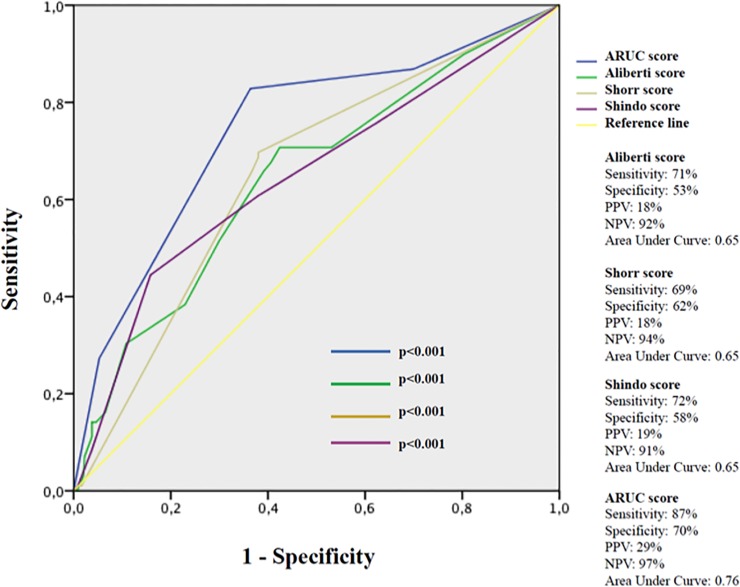
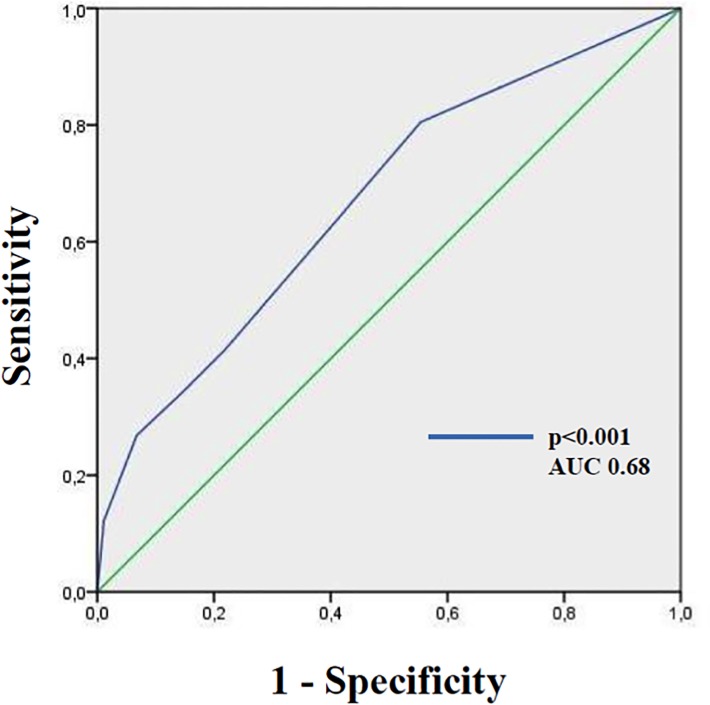
Results: A total of 900 patients were included in the study. The final logistic regression model consisted of four variables: 1) one risk factor for HCAP, 2) bilateral pulmonary infiltration, 3) the presence of pleural effusion, and 4) the severity of respiratory impairment calculated by use of PaO2/FiO2 ratio. A new risk score, the ARUC score, was developed; compared to Aliberti, Shorr, and Shindo scores, this point score system has a good discrimination performance (AUC 0.76, 95% CI 0.71-0.82) and calibration (Hosmer-Lemeshow, χ2 = 7.64; p = 0.469). The new score outperformed HCAP definition in predicting etiology due to MDR organism. The performance of this bedside score was confirmed in the validation cohort (AUC 0.68, 95% CI 0.60-0.77).
Conclusion: Physicians working in ED should adopt simple risk scores, like ARUC score, to select the most appropriate antibiotic regimens. This individualized approach may help clinicians to identify those patients who need an empirical broad-spectrum antibiotic therapy.
Conflict of interest statement
Figures
References
-
- Venditti M, Falcone M, Corrao S, Licata G, Serra P, and the Study Group of the Italian Society of Internal Medicine. Comparison of the outcomes of patients hospitalized with community-acquired, health care–associated, and hospital-acquired pneumonia. Ann Intern Med 2009; 150: 19–26. - PubMed
-
- Kollef MH, Shorr A, Tabak YP, Gupta V, Liu LZ, Johannes RS. Epidemiology and outcomes of health-care-associated pneumonia: results from a large US database of culture-positive pneumonia. Chest 2005;128:3854–62. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
