

Quality of post arrest care does not differ by time of day at a specialized resuscitation center
- PMID: 25860211
- PMCID: PMC4554053
- DOI: 10.1097/MD.0000000000000664
Quality of post arrest care does not differ by time of day at a specialized resuscitation center
Abstract
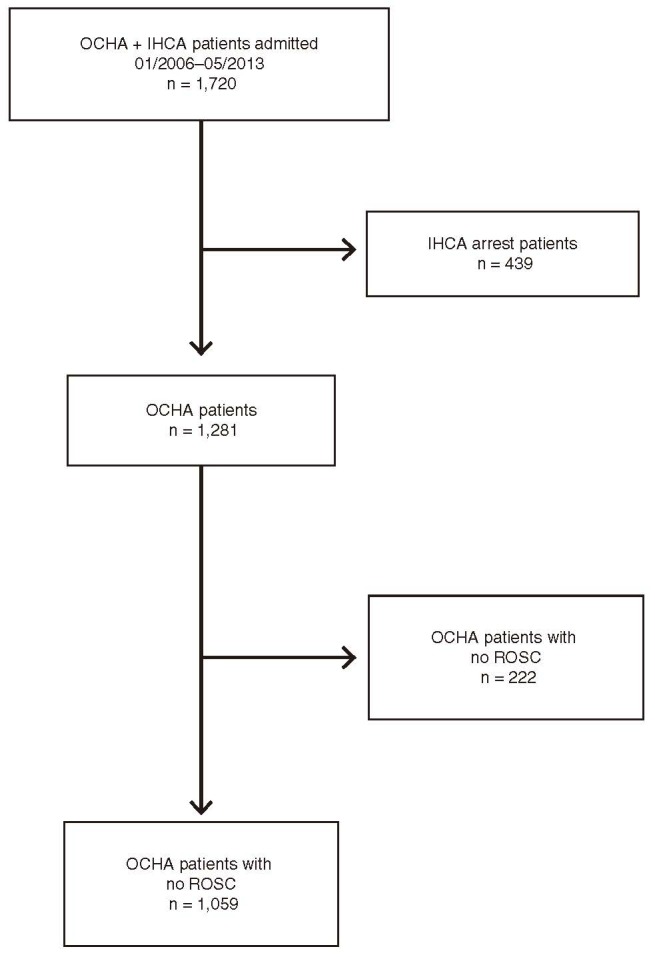
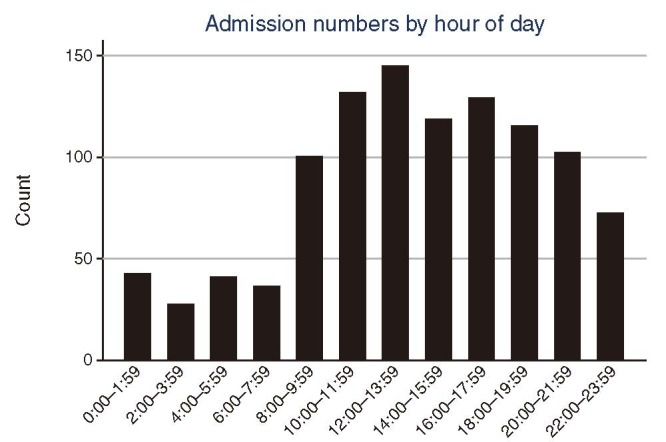
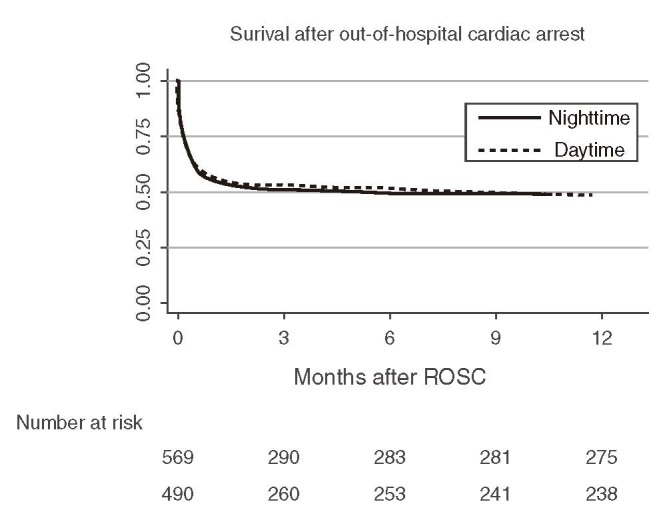
Previous studies suggest worse outcomes after out-of-hospital cardiac arrest (OHCA) at night. We analyzed whether patients admitted after nontraumatic OHCA to a resuscitation center received the same quality post arrest care at day and night and whether quality of care affected clinical outcomes. We analyzed data of OHCA patients with return of spontaneous circulation admitted to the Vienna general hospital emergency department between January 2006 and May 2013. Data reported include admission time (day defined from 8 AM to 4 PM based on staffing), time to initiation of hypothermia, and door-to-balloon time in patients with ST-elevation myocardial infarction. Survival and cognitive performance at 12 months were assessed. In this retrospective observational study, 1059 patients (74% males, n = 784) with a mean age of 58 ± 16 years were analyzed. The vast majority was treated with induced hypothermia (77% of day vs. 79% of night admissions, P = 0.32) within 1 hour of admission (median time admission to cooling 27 (confidence interval [CI]: 10-60) vs. 23 (CI: 11-59) minutes day vs. night, P = 0.99). In 298 patients with ST-elevation myocardial infarction, median door-to-balloon time did not differ between day and night admissions (82 minutes, CI: 60 to 142 for day vs. 86 minutes, CI: 50 to 135 for night, P = 0.36). At 12 months, survival was recorded in 238 of 490 day and 275 of 569 night admissions (49% vs. 48%, P = 0.94%), and a good neurologic outcome was recorded in 210 of 490 day and 231 of 569 night admissions (43% vs. 41%, P = 0.46). Patients admitted to our department after OHCA were equally likely to receive timely high-quality postresuscitation care irrespective of time of day. Survival and good neurologic outcome at 12 months did not differ between day and night admissions. Our results may support the concept of specialized post arrest care centers.
Conflict of interest statement
All other authors declare that they have no conflicts of interest.
Figures
References
-
- McNally B, Robb R, Mehta M, et al. Out-of-hospital cardiac arrest surveillance – Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005–December 31, 2010. MMWR Surveill Summ 2011; 60:1–19. - PubMed
-
- Stromsoe A, Svensson L, Axelsson AB, et al. Improved outcome in Sweden after out-of-hospital cardiac arrest and possible association with improvements in every link in the chain of survival. Eur Heart J 2014; [Epub ahead of print]. - PubMed
-
- Morrison LJ, Deakin CD, Morley PT, et al. Advanced Life Support Chapter Collaborators. Part 8: advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2010; 122:345–421. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
