

Cytokine profiles contribute to understanding the pathogenic difference between Good syndrome and oral lichen planus: two case reports and literature review
- PMID: 25860215
- PMCID: PMC4554038
- DOI: 10.1097/MD.0000000000000704
Cytokine profiles contribute to understanding the pathogenic difference between Good syndrome and oral lichen planus: two case reports and literature review
Abstract
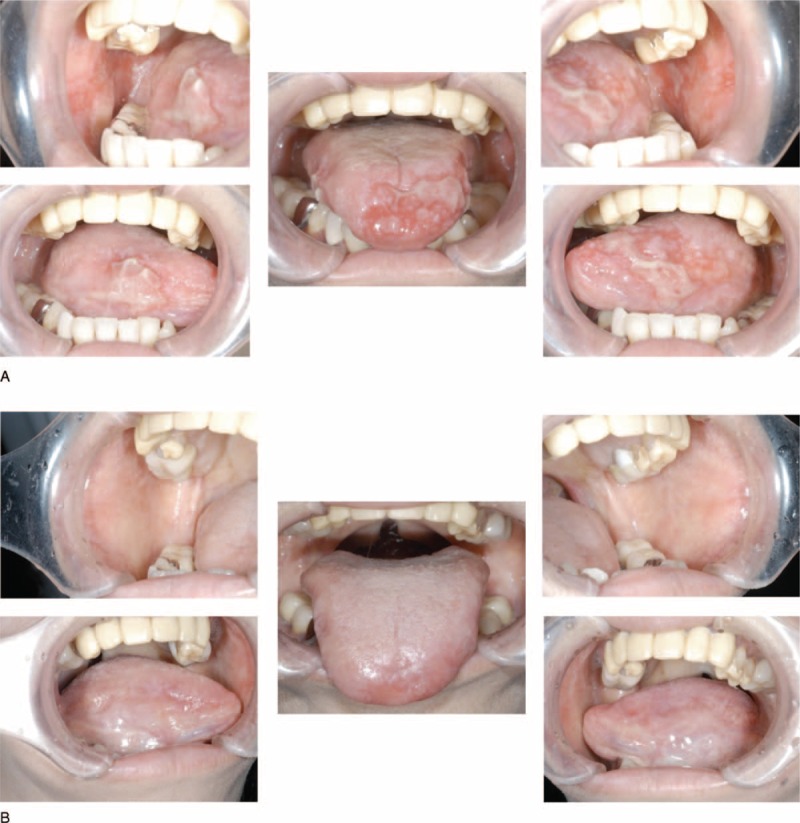
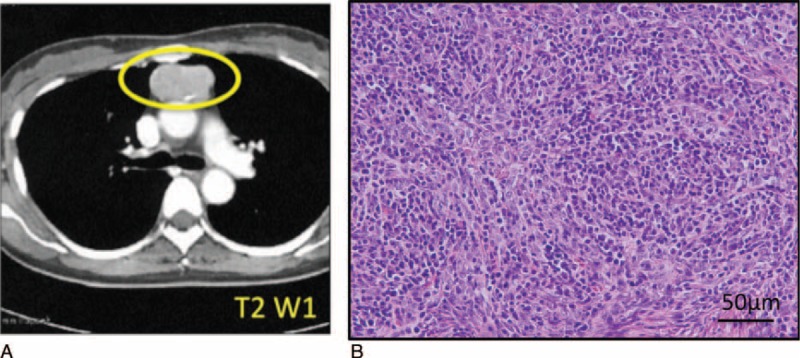
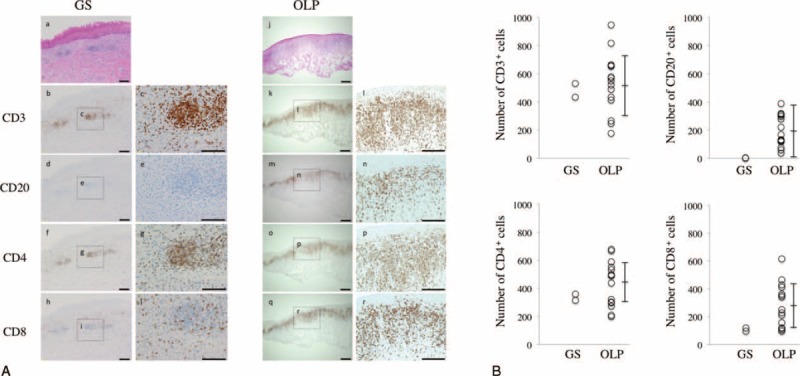
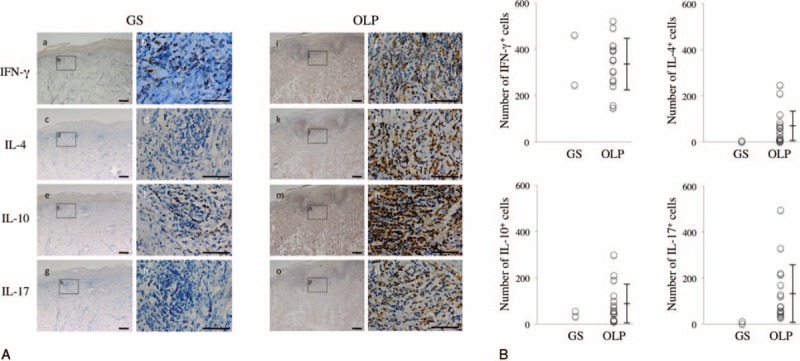
We described and analyzed the pathogenic difference between Good syndrome (GS) and oral lichen planus (OLP) in oral mucosa. Good syndrome (GS) is a rare disease characterized by B and T cell immunodeficiency associated with hypogammaglobulinemia and thymoma. GS patients frequently develop oral lichenoid lesions with lymphocytic infiltration beneath the basal layer. Oral lichen planus (OLP) is a chronic inflammatory disease of the oral mucosa characterized by destruction of basal cells by Langerhans cells, macrophages, and T lymphocytes. Although the histological features of the lesions of both diseases are very similar, the pathogenesis of GS in the oral mucosa remains unknown. In this study, we thus investigated the expression of infiltrating lymphocyte subsets (CD3, CD20, CD4, and CD8) and T helper (Th) cytokines including interferon (IFN)-γ (Th1 type), interleukin (IL)-4 (Th2 type), IL-17 (Th17 type), and IL-10 (regulatory T cell type) by immunohistochemistry in buccal mucosa specimens from 2 GS patients compared with 15 OLP patients. All patients showed a predominance of CD3 T cells over CD20 B cells, and CD4 Th cells over CD8 cytotoxic T cells. This polarization was especially prominent in GS. IFN-γ and IL-10 were strongly detected in the infiltrating lymphocytes of all patients. However, IL-4 and IL-17 were detected in OLP patients only. These results suggest that the pathogenesis of GS is different from that of OLP. GS is a unique inflammatory disorder characterized by dysfunction of Th2 and Th17 immune reactions via abnormal T-B cell interaction.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Myeloid dendritic cells stimulated by thymic stromal lymphopoietin promote Th2 immune responses and the pathogenesis of oral lichen planus.PLoS One. 2017 Mar 9;12(3):e0173017. doi: 10.1371/journal.pone.0173017. eCollection 2017. PLoS One. 2017. PMID: 28278185 Free PMC article.
-
Role of distinct CD4(+) T helper subset in pathogenesis of oral lichen planus.J Oral Pathol Med. 2016 Jul;45(6):385-93. doi: 10.1111/jop.12405. Epub 2015 Dec 23. J Oral Pathol Med. 2016. PMID: 26693958 Review.
-
Distinct interferon-gamma and interleukin-9 expression in cutaneous and oral lichen planus.J Eur Acad Dermatol Venereol. 2017 May;31(5):880-886. doi: 10.1111/jdv.13989. Epub 2016 Oct 21. J Eur Acad Dermatol Venereol. 2017. PMID: 27696572
-
Cytokines Levels and Salivary Microbiome Play A Potential Role in Oral Lichen Planus Diagnosis.Sci Rep. 2019 Dec 2;9(1):18137. doi: 10.1038/s41598-019-54615-y. Sci Rep. 2019. PMID: 31792433 Free PMC article.
-
The potential roles of Th17 cells in the pathogenesis of oral lichen planus.Inflamm Res. 2023 Jul;72(7):1513-1524. doi: 10.1007/s00011-023-01763-7. Epub 2023 Jul 6. Inflamm Res. 2023. PMID: 37414985 Review.
Cited by
-
Myeloid dendritic cells stimulated by thymic stromal lymphopoietin promote Th2 immune responses and the pathogenesis of oral lichen planus.PLoS One. 2017 Mar 9;12(3):e0173017. doi: 10.1371/journal.pone.0173017. eCollection 2017. PLoS One. 2017. PMID: 28278185 Free PMC article.
-
Oral Lichen Planus in Patients With Good's Syndrome: A Literature Review.Cureus. 2023 Feb 19;15(2):e35177. doi: 10.7759/cureus.35177. eCollection 2023 Feb. Cureus. 2023. PMID: 36960269 Free PMC article. Review.
-
Induction of High Endothelial Venule-like Vessels in Oral and Cutaneous Lichen Planus: A Comparative Study.J Histochem Cytochem. 2020 May;68(5):343-350. doi: 10.1369/0022155420923272. J Histochem Cytochem. 2020. PMID: 32391737 Free PMC article.
-
Oral lichen planus - case report.Rom J Morphol Embryol. 2020 Apr-Jun;61(2):563-567. doi: 10.47162/RJME.61.2.28. Rom J Morphol Embryol. 2020. PMID: 33544810 Free PMC article.
-
When the Good Syndrome Goes Bad: A Systematic Literature Review.Front Immunol. 2021 May 25;12:679556. doi: 10.3389/fimmu.2021.679556. eCollection 2021. Front Immunol. 2021. PMID: 34113351 Free PMC article.
References
-
- Lodi G, Scully C, Carrozzo M, et al. Current controversies in oral lichen planus: report of an international consensus meeting. Part 1. Viral infections and etiopathogenesis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005; 100:40–51. - PubMed
-
- Sugerman PB, Savage NW, Seymour GJ. Phenotype and suppressor activity of T-lymphocyte clones extracted from lesions of oral lichen planus. Br J Dermatol 1994; 131:319–324. - PubMed
-
- Kawamura E, Nakamura S, Sasaki M, et al. Accumulation of oligoclonal T cells in the infiltrating lymphocytes in oral lichen planus. J Oral Pathol Med 2003; 32:282–289. - PubMed
-
- Miyakis S, Pefanis A, Passam FH, et al. Thymoma with immunodeficiency (Good's syndrome): review of the literature apropos three cases. Scand J Infect Dis 2006; 38:314–319. - PubMed
-
- Good RA, Varco RL. A clinical and experimental study of agammaglobulinemia. J Lancet 1955; 75:245–271. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
