

Intraoperative computed tomography versus Perdriolle and scoliometer evaluation of spine rotation in adolescent idiopathic scoliosis
- PMID: 25861628
- PMCID: PMC4377381
- DOI: 10.1155/2015/460340
Intraoperative computed tomography versus Perdriolle and scoliometer evaluation of spine rotation in adolescent idiopathic scoliosis
Abstract
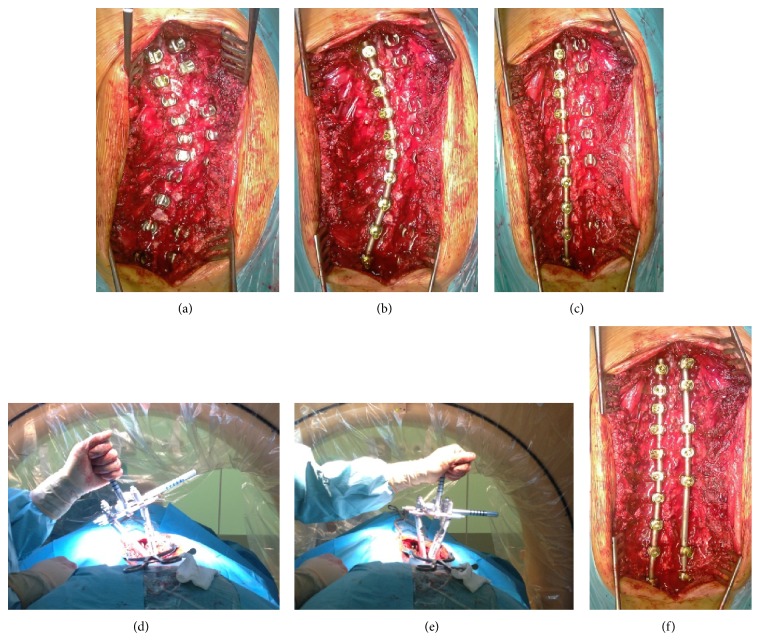
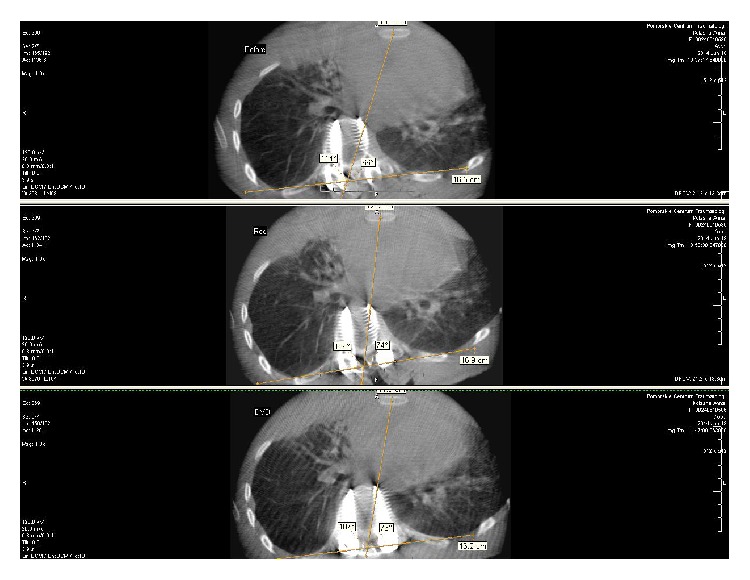
Numerous indirect methods for apical vertebral rotation (AVR) measurement have been reported and none of them seems to be as accurate as computed tomography evaluation. The aim of this study was to compare spinal rotation changes during innovative technique of intraoperative computed tomography (ICT) evaluation with indirect methods such as Perdriolle and clinical evaluation with scoliometer. We examined 42 adolescent idiopathic scoliosis (AIS) patients treated with posterior scoliosis surgery (PSS). The mean age at the time of surgery was 16 years. ICT evaluation was performed before and after scoliosis correction in prone position. Clinical rib hump measure with scoliometer and radiographic Perdriolle were performed before and after surgery. There was 71,5% of average rib hump correction with scoliometer but only 31% of correction with ICT (P=0,026) and there was no significant correlation between them (R=0,297, p=0,26). Mean postcorrectional Perdriolle AVR had a decrease of 16,5°. The average ICT AVR had a decrease of only 1,2° (P=0,003). There was no significant statistic correlation between ICT and Perdriolle AVR evaluation (R=0,297, p=0,2). There is a significant discrepancy in AVR and rib hump assessment between scoliometer and Perdriolle methods and ICT evaluation, which seems to be the most accurate tool for spinal derotation measurement.
Figures






References
-
- Cobb J. R. Outlines for the study of scoliosis. Instructional Course Lectures. 1948:261–275.
-
- Pankowski R., Roclawski M., Smoczynski A., et al. he influence of the development of scoliosis posterior surgery on 3-planar deformity correction. Research into Spinal Deformities. 2012;8:p. 492.
-
- Nash C. L., Jr., Moe J. H. A study of vertebral rotation. The Journal of Bone & Joint Surgery—American Volume. 1969;51(2):223–229. - PubMed
-
- Perdriolle R., Vidal J. Morphology of scoliosis: three-dimensional evolution. Orthopedics. 1987;10(6):909–915. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
