

Associations of Posthemodialysis Weights above and below Target Weight with All-Cause and Cardiovascular Mortality
- PMID: 25862779
- PMCID: PMC4422248
- DOI: 10.2215/CJN.10201014
Associations of Posthemodialysis Weights above and below Target Weight with All-Cause and Cardiovascular Mortality
Abstract
Background and objectives: Fluid removal via ultrafiltration is a primary function of hemodialysis, and inadequate volume control is associated with significant morbidity and mortality among chronic dialysis patients. Treatment-to-treatment fluid removal goals are typically calculated on the basis of interdialytic weight gain and prescribed target weight. The clinical effect of frequent missed target weights is unclear. This study was designed to evaluate the associations of postdialysis weights above and below the prescribed target weight (separately) and outcomes.
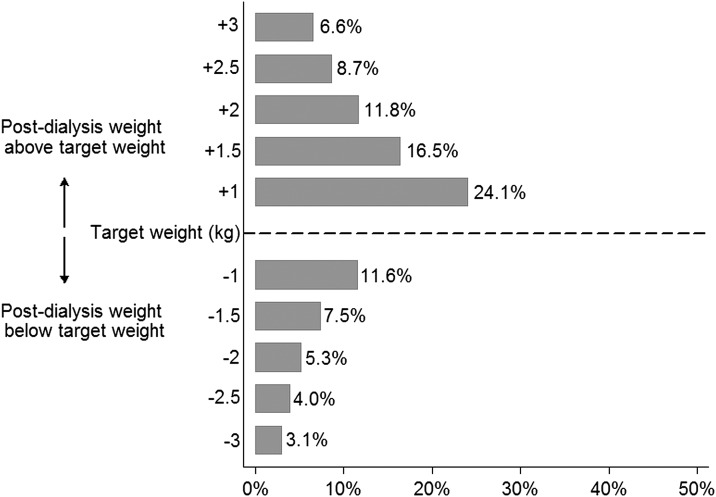
Design, setting, participants, & measurements: Data were taken from a national cohort of 10,785 prevalent, thrice-weekly, in-center hemodialysis patients dialyzing from 2005 to 2008 (median time at risk, 2.1 [25th percentile, 75th percentile] years) at a single dialysis organization. Patients were characterized as having an above target weight miss if their postdialysis weight was >2 kg above target weight in at least 30% of baseline treatments (14.6% of cohort), or they were characterized as control otherwise. Below target weight miss characterization was analogous for patients with postdialysis weight >2 kg below target weight (6.6% of cohort). Coprimary endpoints were all-cause and cardiovascular mortality.
Results: Above target weight miss in at least 30% of treatments (versus not) was associated with greater all-cause mortality (adjusted hazard ratio, 1.28; 95% confidence interval, 1.15 to 1.43); and below target weight miss in at least 30% of treatments (versus not) was associated with greater all-cause mortality (adjusted hazard ratio, 1.22; 95% confidence interval, 1.05 to 1.40). Both above and below target weight misses were also significantly associated with greater cardiovascular mortality. Secondary analyses demonstrated dose-response relationships between target weight misses and mortality. Results from sensitivity analyses considering the difference in postdialysis and target weights as a proportion of body weight were analogous to the primary results.
Conclusions: Postdialysis weights >2 kg above and below target weight are associated with higher all-cause and cardiovascular mortality. Consistent target weight achievement is a viable target for improving fluid management.
Keywords: cardiovascular; chronic hemodialysis; clinical epidemiology.
Copyright © 2015 by the American Society of Nephrology.
Figures

Comment in
-
Posthemodialysis weights and mortality: another narrow range target?Clin J Am Soc Nephrol. 2015 May 7;10(5):729-31. doi: 10.2215/CJN.03110315. Epub 2015 Apr 10. Clin J Am Soc Nephrol. 2015. PMID: 25862780 Free PMC article. No abstract available.
References
-
- Saran R, Bragg-Gresham JL, Levin NW, Twardowski ZJ, Wizemann V, Saito A, Kimata N, Gillespie BW, Combe C, Bommer J, Akiba T, Mapes DL, Young EW, Port FK: Longer treatment time and slower ultrafiltration in hemodialysis: Associations with reduced mortality in the DOPPS. Kidney Int 69: 1222–1228, 2006 - PubMed
-
- Zoccali C, Benedetto FA, Tripepi G, Mallamaci F: Cardiac consequences of hypertension in hemodialysis patients. Semin Dial 17: 299–303, 2004 - PubMed
-
- Sharpe N: Left ventricular remodeling: Pathophysiology and treatment. Heart Fail Monit 4: 55–61, 2003 - PubMed
-
- Burton JO, Korsheed S, Grundy BJ, McIntyre CW: Hemodialysis-induced left ventricular dysfunction is associated with an increase in ventricular arrhythmias. Ren Fail 30: 701–709, 2008 - PubMed
