

Predicting high-grade cancer at ten-core prostate biopsy using four kallikrein markers measured in blood in the ProtecT study
- PMID: 25863334
- PMCID: PMC4554254
- DOI: 10.1093/jnci/djv095
Predicting high-grade cancer at ten-core prostate biopsy using four kallikrein markers measured in blood in the ProtecT study
Abstract
Background: Many men with elevated prostate-specific antigen (PSA) levels in serum do not have aggressive prostate cancer and undergo unnecessary biopsy. Retrospective studies using cryopreserved serum suggest that four kallikrein markers can predict biopsy outcome.
Methods: Free, intact and total PSA, and kallikrein-related peptidase 2 were measured in cryopreserved blood from 6129 men with elevated PSA (≥3.0ng/mL) participating in the prospective, randomized trial Prostate Testing for Cancer and Treatment. Marker levels from 4765 men providing anticoagulated plasma were incorporated into statistical models to predict any-grade and high-grade (Gleason score ≥7) prostate cancer at 10-core biopsy. The models were corrected for optimism by 10-fold cross validation and independently validated using markers measured in serum from 1364 men. All statistical tests were two-sided.
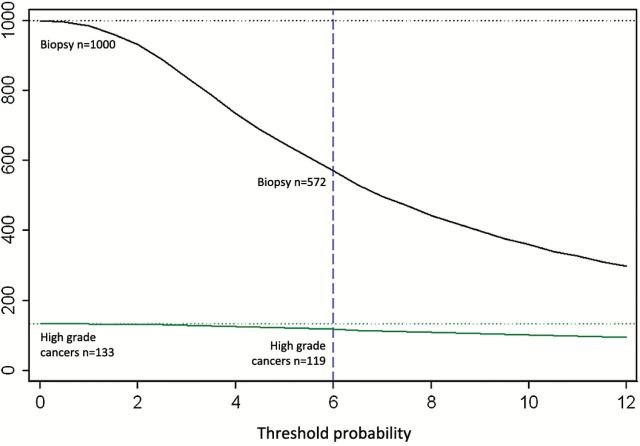
Results: The four kallikreins enhanced prostate cancer detection compared with PSA and age alone. Area under the curve (AUC) for the four kallikreins was 0.719 (95% confidence interval [CI] = 0.704 to 0.734) vs 0.634 (95% CI = 0.617 to 0.651, P < .001) for PSA and age alone for any-grade cancer, and 0.820 (95% CI = 0.802 to 0.838) vs 0.738 (95% CI = 0.716 to 0.761) for high-grade cancer. Using a 6% risk of high-grade cancer as an illustrative cutoff, for 1000 biopsied men with PSA levels of 3.0ng/mL or higher, the model would reduce the need for biopsy in 428 men, detect 119 high-grade cancers, and delay diagnosis of 14 of 133 high-grade cancers. Models exhibited excellent discrimination on independent validation among men with only serum samples available for analysis.
Conclusions: A statistical model based on kallikrein markers was validated in a large prospective study and reduces unnecessary biopsies while delaying diagnosis of high-grade cancers in few men.
© The Author 2015. Published by Oxford University Press.
Figures
Comment in
-
Re: Predicting High-Grade Cancer at Ten-Core Prostate Biopsy Using Four Kallikrein Markers Measured in Blood in the ProtecT Study.J Urol. 2015 Dec;194(6):1632. doi: 10.1016/j.juro.2015.09.014. Epub 2015 Sep 8. J Urol. 2015. PMID: 26582666 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
