

Ambulatory respiratory rate trends identify patients at higher risk of worsening heart failure in implantable cardioverter defibrillator and biventricular device recipients: a novel ambulatory parameter to optimize heart failure management
- PMID: 25863797
- PMCID: PMC4438200
- DOI: 10.1007/s10840-015-9983-6
Ambulatory respiratory rate trends identify patients at higher risk of worsening heart failure in implantable cardioverter defibrillator and biventricular device recipients: a novel ambulatory parameter to optimize heart failure management
Abstract
Purpose: Respiratory distress is the primary driver for heart failure (HF) hospitalization. Implantable pacemakers and defibrillators are capable of monitoring respiratory rate (RR) in ambulatory HF patients. We investigated changes in RR prior to HF hospitalizations and its near-term risk stratification power.
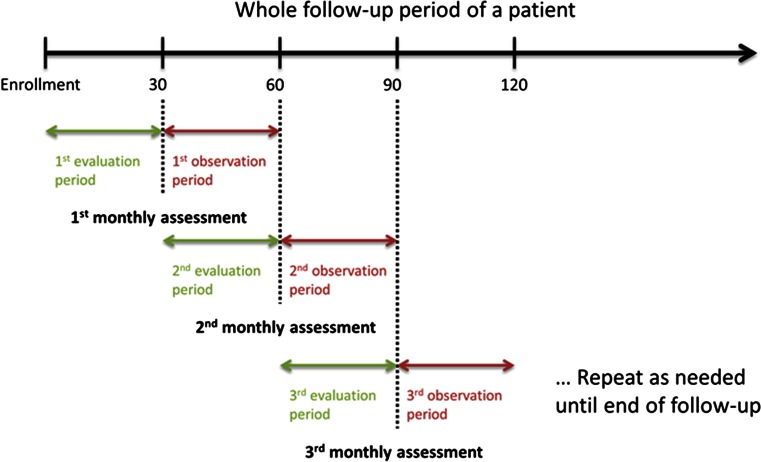
Methods: NOTICE-HF was an international multi-center study. Patients were implanted with an implantable cardioverter defibrillator or cardiac resynchronization therapy defibrillator, capable of trending daily maximum, median, and minimum RR (maxRR, medRR, minRR). RR from 120 patients with 9 months of follow-up was analyzed. One-tailed Student's t test was used to compare RR values prior to HF events to baseline defined as 4 weeks prior to the events. A Cox regression model was used to calculate the hazard ratios (HR) for the 30-day HF hospitalization risk based on RR values in the preceding month.
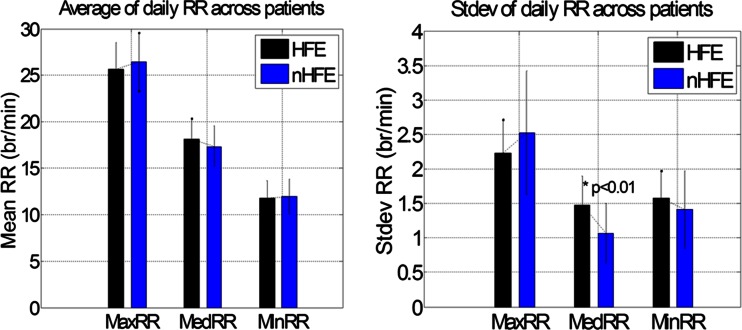
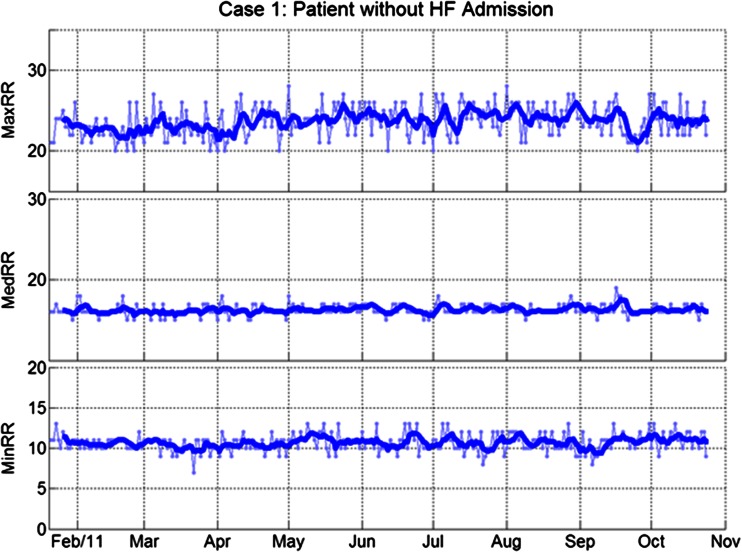
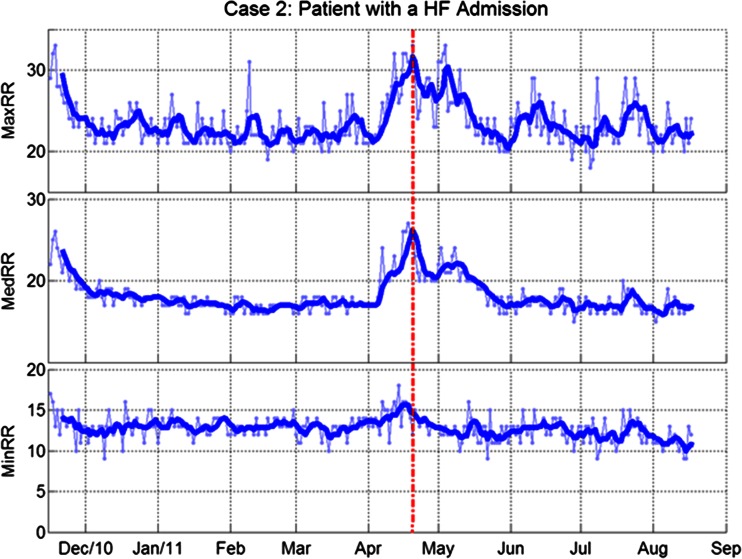
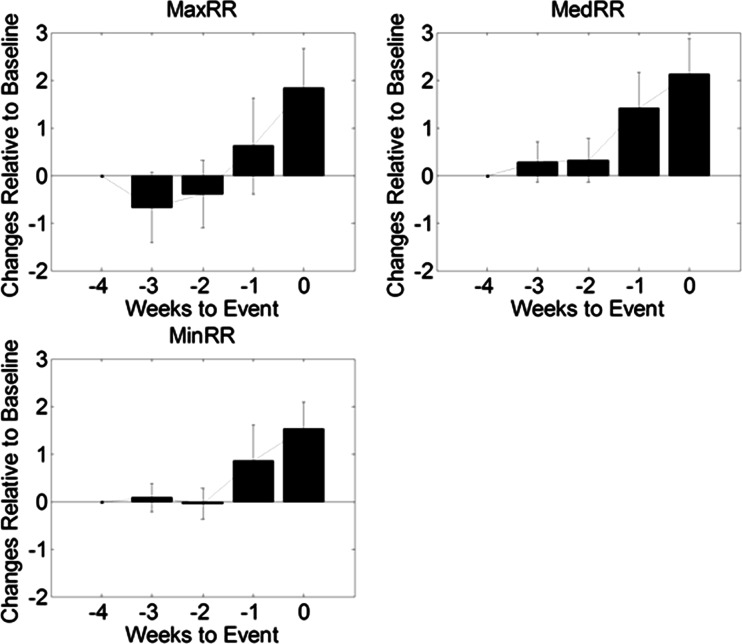
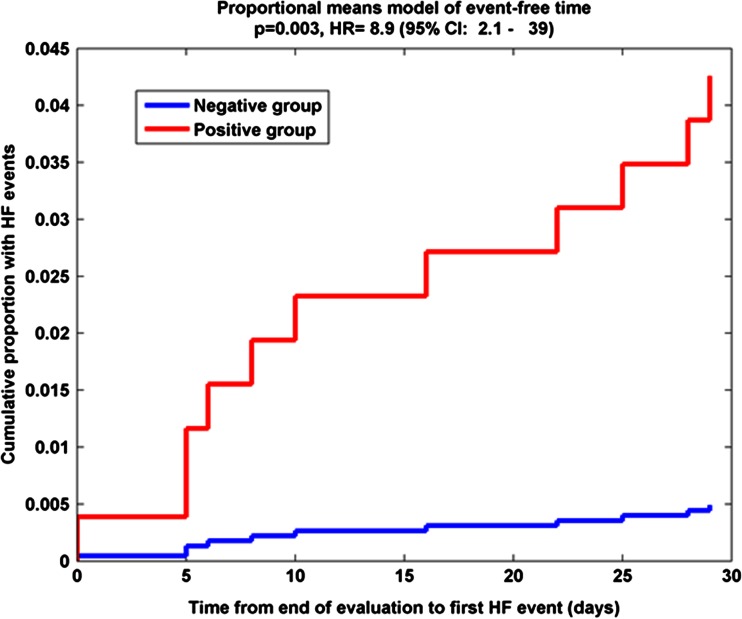
Results: Daily maxRR, medRR, and minRR were significantly elevated prior to HF events compared to baseline (ΔmaxRR 1.8 ± 3.0; p = 0.02; ΔmedRR, 2.1 ± 2.8; p = 0.007; ΔminRR, 1.5 ± 2.1, p = 0.008). Risk of experiencing HF events within 30-days was increased if the standard deviation of medRR over the preceding month was above 1.0 br/min (HR = 12.3, 95 % confidence interval (CI) 2.57-59, p = 0.002). The risk remained high after adjusting for clinical variables that differed at enrollment.
Conclusion: Ambulatory daily respiratory rate trends may be a valuable addition to standard management for HF patients.
Figures
References
-
- Braunwald E, Colucci W, Grossman W. Clinical aspects of heart failure: high-output heart failure; pulmonary edema. In: Braunwald E, editor. Heart Diseases. 5. New York: WB Saunders; 1997. pp. 464–465.
-
- Fonarow GC, ADHERE. Scientific Advisory Committee The Acute Decompensated Heart Failure National Registry (ADHERE): opportunities to improve care of patients hospitalized with acute decompensated heart failure. Reviews in Cardiovascular Medicine. 2003;4(Suppl 7):S21–S30. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
