

Lymphoma incidence, survival and prevalence 2004-2014: sub-type analyses from the UK's Haematological Malignancy Research Network
- PMID: 25867256
- PMCID: PMC4453686
- DOI: 10.1038/bjc.2015.94
Lymphoma incidence, survival and prevalence 2004-2014: sub-type analyses from the UK's Haematological Malignancy Research Network
Abstract
Background: Population-based information about cancer occurrence and survival are required to inform clinical practice and research; but for most lymphomas data are lacking.
Methods: Set within a socio-demographically representative UK population of nearly 4 million, lymphoma data (N=5796) are from an established patient cohort.
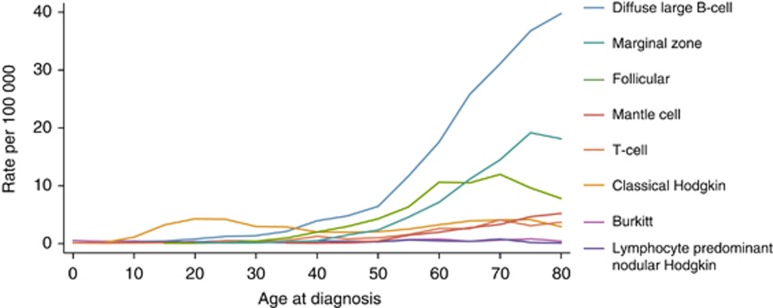
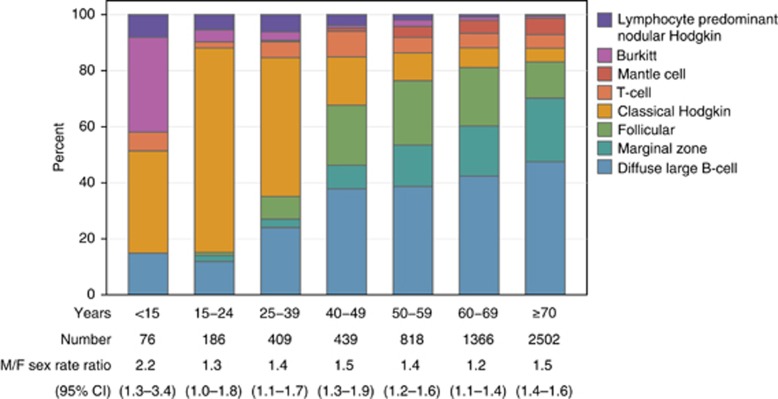
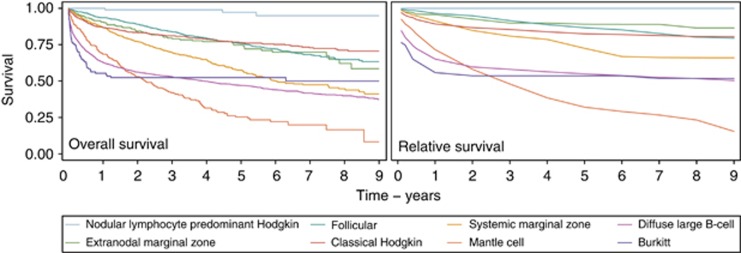
Results: Incidence, survival (overall and relative) and prevalence estimates for >20 subtypes are presented. With few exceptions, males tended to be diagnosed at younger ages and have significantly (P<0.05) higher incidence rates. Differences were greatest at younger ages: the <15 year male/female rate ratio for all subtypes combined being 2.2 (95% CI 1.3-3.4). These gender differences impacted on prevalence; most subtype estimates being significantly (P<0.05) higher in males than females. Outcome varied widely by subtype; survival of patients with nodular lymphocyte predominant Hodgkin lymphoma approached that of the general population, whereas less than a third of those with other B-cell (e.g., mantle cell) or T-cell (e.g., peripheral-T) lymphomas survived for ≥5 years. No males/female survival differences were detected.
Conclusions: Major strengths of our study include completeness of ascertainment, world-class diagnostics and generalisability. The marked variations demonstrated confirm the requirement for 'real-world' data to inform aetiological hypotheses, health-care planning and the future monitoring of therapeutic changes.
Figures

References
-
- Al-Refaie WB, Vickers SM, Zhong W, Parsons H, Rothenberger D, Habermann EB. Cancer trials versus the real world in the United States. Ann Surg. 2011;254:438–442. - PubMed
-
- Cancer Research UK (2006) Cancer Survival Group Strel (v.1.2.7) computer program and life tables for cancer survival analysis.
-
- Crouch S, Smith A, Painter D, Li J, Roman E. Determining disease prevalence from incidence and survival using simulation techniques. Cancer Epidemiol. 2014;38:193–199. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
