

Paradigm Shifts in Atherosclerotic Renovascular Disease: Where Are We Now?
- PMID: 25868641
- PMCID: PMC4552124
- DOI: 10.1681/ASN.2014121274
Paradigm Shifts in Atherosclerotic Renovascular Disease: Where Are We Now?
Abstract
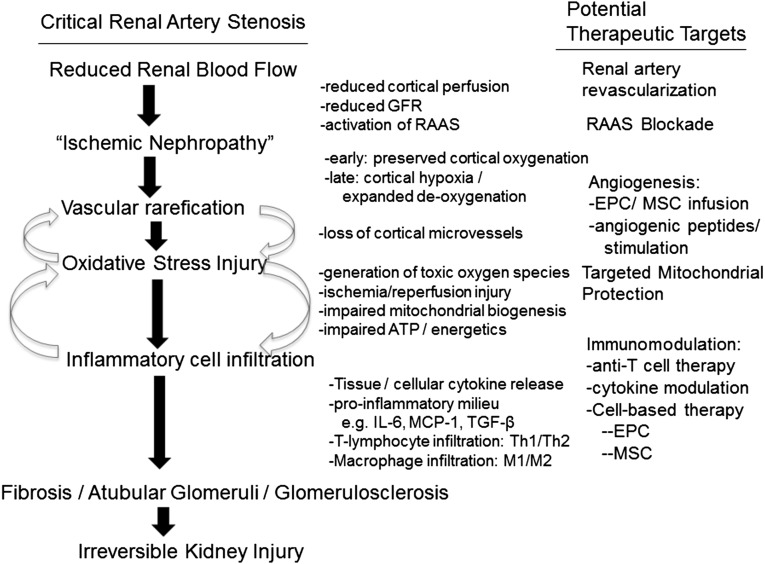
Results of recent clinical trials and experimental studies indicate that whereas atherosclerotic renovascular disease can accelerate both systemic hypertension and tissue injury in the poststenotic kidney, restoring vessel patency alone is insufficient to recover kidney function for most subjects. Kidney injury in atherosclerotic renovascular disease reflects complex interactions among vascular rarefication, oxidative stress injury, and recruitment of inflammatory cellular elements that ultimately produce fibrosis. Classic paradigms for simply restoring blood flow are shifting to implementation of therapy targeting mitochondria and cell-based functions to allow regeneration of vascular, glomerular, and tubular structures sufficient to recover, or at least stabilize, renal function. These developments offer exciting possibilities of repair and regeneration of kidney tissue that may limit progressive CKD in atherosclerotic renovascular disease and may apply to other conditions in which inflammatory injury is a major common pathway.
Keywords: macrophages; mesangial cells; oxidative stress; renal artery stenosis.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- Textor SC: Atherosclerotic renal artery stenosis: Overtreated but underrated? J Am Soc Nephrol 19: 656–659, 2008 - PubMed
-
- Murphy TP, Soares G, Kim M: Increase in utilization of percutaneous renal artery interventions by medicare beneficiaries, 1996-2000. AJR Am J Roentgenol 183: 561–568, 2004 - PubMed
-
- Balk E, Raman G, Chung M, Ip S, Tatsioni A, Alonso A, Chew P, Gilbert SJ, Lau J: Effectiveness of management strategies for renal artery stenosis: A systematic review. Ann Intern Med 145: 901–912, 2006 - PubMed
-
- Ritchie J, Green D, Chrysochou C, Chalmers N, Foley RN, Kalra PA: High-risk clinical presentations in atherosclerotic renovascular disease: Prognosis and response to renal artery revascularization. Am J Kidney Dis 63: 186–197, 2014 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
