

Immunogenicity, safety, and tolerability of 13-valent pneumococcal conjugate vaccine followed by 23-valent pneumococcal polysaccharide vaccine in recipients of allogeneic hematopoietic stem cell transplant aged ≥2 years: an open-label study
- PMID: 25870329
- PMCID: PMC4503811
- DOI: 10.1093/cid/civ287
Immunogenicity, safety, and tolerability of 13-valent pneumococcal conjugate vaccine followed by 23-valent pneumococcal polysaccharide vaccine in recipients of allogeneic hematopoietic stem cell transplant aged ≥2 years: an open-label study
Abstract
Background: Life-threatening Streptococcus pneumoniae infections often occur after hematopoietic stem cell transplant (HSCT); vaccination is important for prevention.
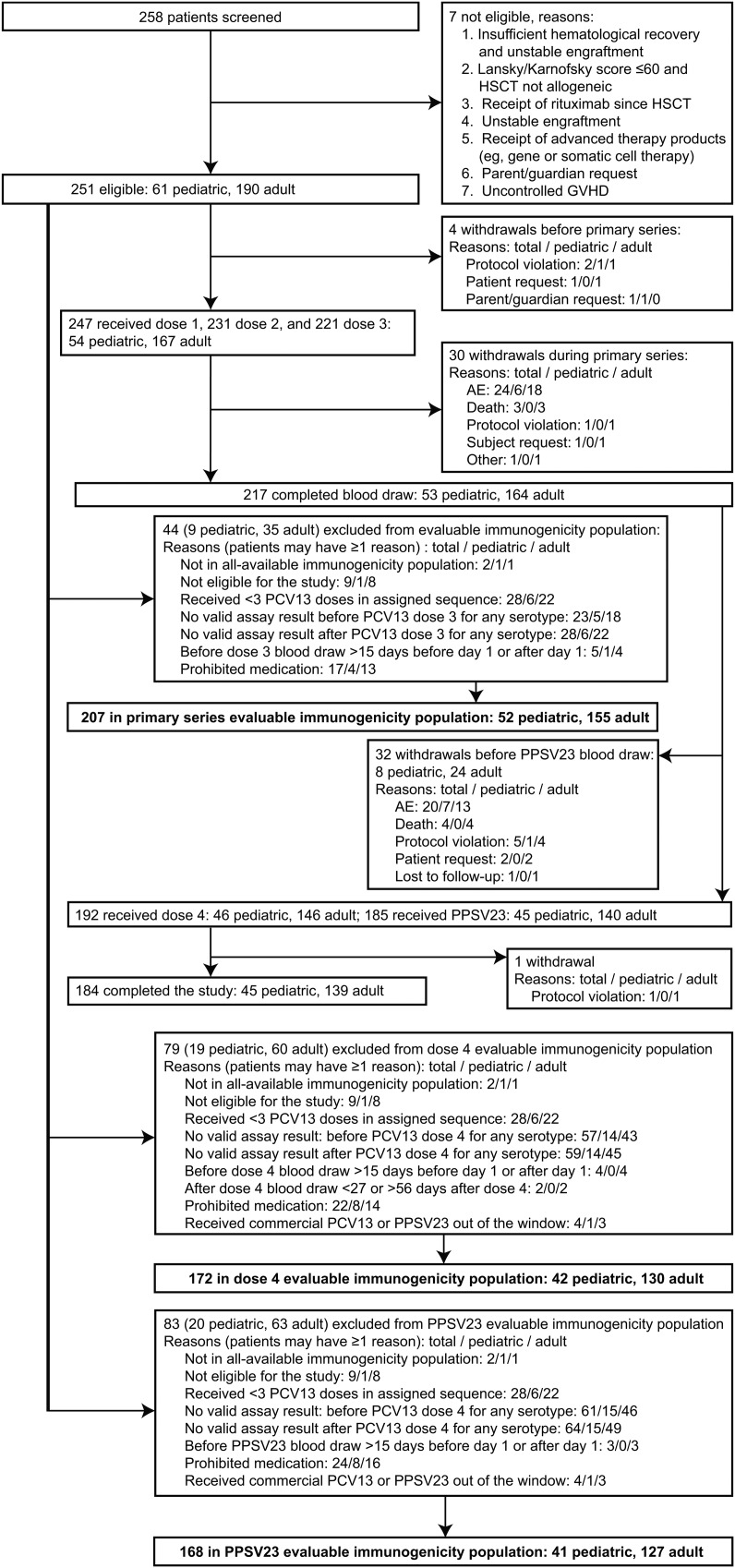
Methods: In an open-label study, patients (n = 251) 3-6 months after allogeneic HSCT received 3 doses of 13-valent pneumococcal conjugate vaccine (PCV13) at 1-month intervals, a fourth dose 6 months later, and 1 dose of 23-valent pneumococcal polysaccharide vaccine (PPSV23) 1 month later. Immunogenicity at prespecified time points and vaccine safety were assessed.
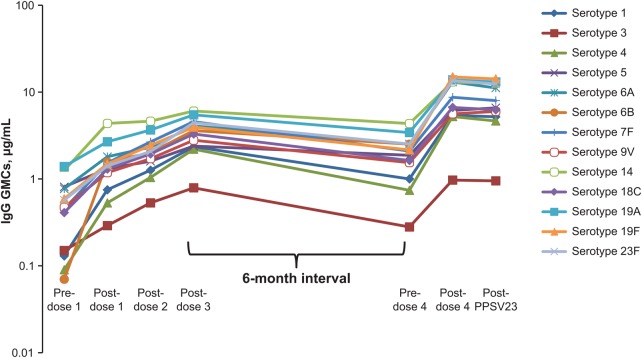
Results: In the evaluable immunogenicity population (N = 216; mean age, 37.8 years), geometric mean fold rises (GMFRs) of immunoglobulin G geometric mean concentrations from baseline to postdose 3 showed significant increases in antibody levels across all PCV13 serotypes (GMFR range, 2.99-23.85; 95% confidence interval lower limit, >1); there were significant declines over the next 6 months, significant increases from predose 4 to postdose 4 (GMFR range, 3.00-6.97), and little change after PPSV23 (GMFR range, 0.86-1.12). Local and systemic reactions were more frequent after dose 4. Six patients experienced serious adverse events possibly related to PCV13 (facial diplegia, injection-site erythema and pyrexia, autoimmune hemolytic anemia, and suspected lack of vaccine efficacy after dose 3 leading to pneumococcal infection), PCV13 and PPSV23 (Guillain-Barré syndrome), or PPSV23 (cellulitis). There were 14 deaths, none related to study vaccines.
Conclusions: A 3-dose PCV13 regimen followed by a booster dose may be required to protect against pneumococcal disease in HSCT recipients. Dose 4 was associated with increased local and systemic reactions, but the overall safety profile of a 4-dose regimen was considered acceptable.
Clinical trials registration: NCT00980655.
Keywords: 13-valent pneumococcal conjugate vaccine; 23-valent pneumococcal polysaccharide vaccine; Streptococcus pneumoniae infections; hematopoietic stem cell transplant.
© The Author 2015. Published by Oxford University Press on behalf of the Infectious Diseases Society of America.
Figures
References
-
- Engelhard D, Cordonnier C, Shaw PJ et al. Early and late invasive pneumococcal infection following stem cell transplantation: a European Bone Marrow Transplantation survey. Br J Haematol 2002; 117:444–50. - PubMed
-
- Kumar D, Humar A, Plevneshi A et al. Invasive pneumococcal disease in adult hematopoietic stem cell transplant recipients: a decade of prospective population-based surveillance. Bone Marrow Transplant 2008; 41:743–7. - PubMed
-
- Torda A, Chong Q, Lee A et al. Invasive pneumococcal disease following adult allogeneic hematopoietic stem cell transplantation. Transpl Infect Dis 2014; 16:751–9. - PubMed
-
- Centers for Disease Control and Prevention. Guidelines for preventing opportunistic infections among hematopoietic stem cell transplant recipients: recommendations of CDC, the Infectious Disease Society of America, and the American Society of Blood and Marrow Transplantation. MMWR Recomm Rep 2000; 49(RR-10):1–127. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
