

Histoplasmosis complicating tumor necrosis factor-α blocker therapy: a retrospective analysis of 98 cases
- PMID: 25870331
- PMCID: PMC4796723
- DOI: 10.1093/cid/civ299
Histoplasmosis complicating tumor necrosis factor-α blocker therapy: a retrospective analysis of 98 cases
Abstract
Background: Histoplasmosis may complicate tumor necrosis factor (TNF)-α blocker therapy. Published case series provide limited guidance on disease management. We sought to determine the need for long-term antifungal therapy and the safety of resuming TNF-α blocker therapy after successful treatment of histoplasmosis.
Methods: We conducted a multicenter retrospective review of 98 patients diagnosed with histoplasmosis between January 2000 and June 2011. Multivariate logistic regression was used to evaluate risk factors for severe disease.
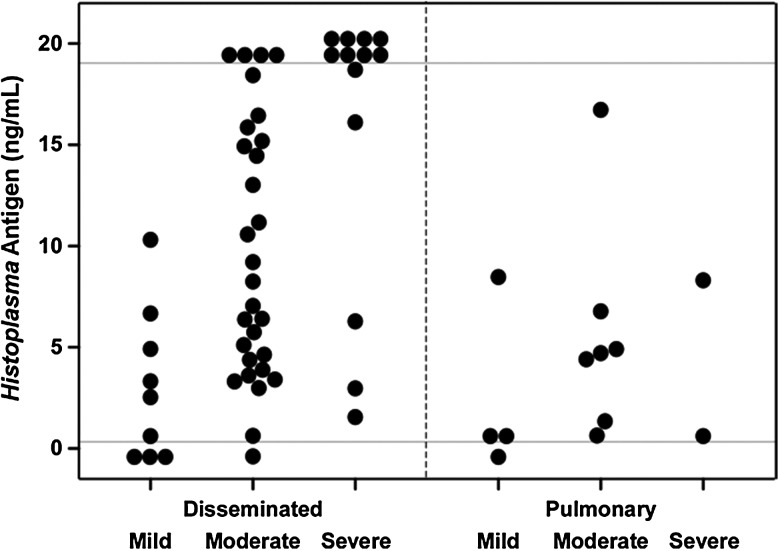
Results: The most commonly used biologic agent was infliximab (67.3%). Concomitant corticosteroid use (odds ratio [OR], 3.94 [95% confidence interval {CI}, 1.06-14.60]) and higher urine Histoplasma antigen levels (OR, 1.14 [95% CI, 1.03-1.25]) were found to be independent predictors of severe disease. Forty-six (47.4%) patients were initially treated with an amphotericin B formulation for a median duration of 2 weeks. Azole treatment was given for a median of 12 months. TNF-α blocker therapy was initially discontinued in 95 of 98 (96.9%) patients and later resumed in 25 of 74 (33.8%) patients at a median of 12 months (range, 1-69 months). The recurrence rate was 3.2% at a median follow-up period of 32 months. Of the 3 patients with recurrence, 2 had restarted TNF-α blocker therapy, 1 of whom died. Mortality rate was 3.2%.
Conclusions: In this study, disease outcomes were generally favorable. Discontinuation of antifungal treatment after clinical response and an appropriate duration of therapy, probably at least 12 months, appears safe if pharmacologic immunosuppression has been held. Resumption of TNF-α blocker therapy also appears safe, assuming that the initial antifungal therapy was administered for 12 months.
Keywords: adalimumab; etanercept; histoplasmosis; immune reconstitution syndrome; infliximab.
© The Author 2015. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Allendoerfer R, Deepe GS., Jr Blockade of endogenous TNF-alpha exacerbates primary and secondary pulmonary histoplasmosis by differential mechanisms. J Immunol 1998; 160:6072–82. - PubMed
-
- Wood KL, Hage CA, Knox KS, et al. Histoplasmosis after treatment with anti-tumor necrosis factor-alpha therapy. Am J Respir Crit Care Med 2003; 167:1279–82. - PubMed
-
- Deepe GS., Jr Modulation of infection with Histoplasma capsulatum by inhibition of tumor necrosis factor-alpha activity. Clin Infect Dis 2005; 41(suppl 3):S204–7. - PubMed
-
- Furst DE, Wallis R, Broder M, Beenhouwer DO. Tumor necrosis factor antagonists: different kinetics and/or mechanisms of action may explain differences in the risk for developing granulomatous infection. Semin Arthritis Rheum 2006; 36:159–67. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
