

Human granulocytic anaplasmosis in the United States from 2008 to 2012: a summary of national surveillance data
- PMID: 25870428
- PMCID: PMC4497906
- DOI: 10.4269/ajtmh.15-0122
Human granulocytic anaplasmosis in the United States from 2008 to 2012: a summary of national surveillance data
Abstract
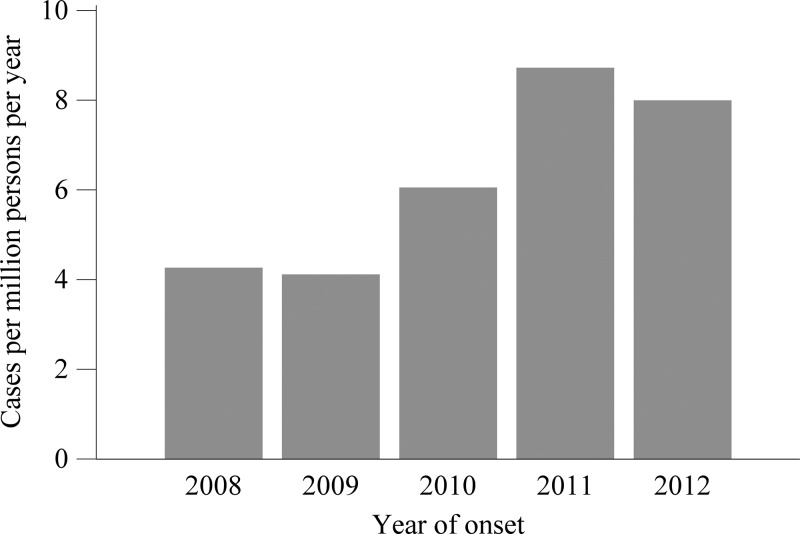
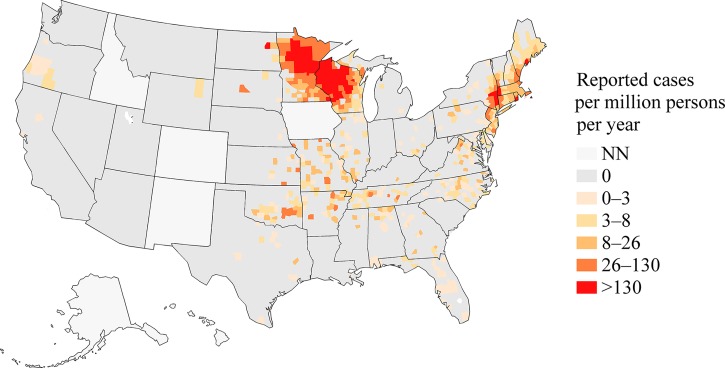
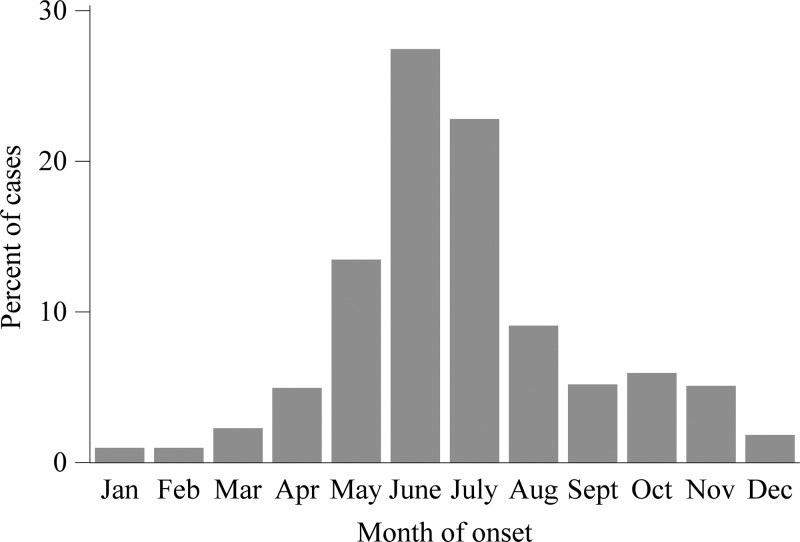
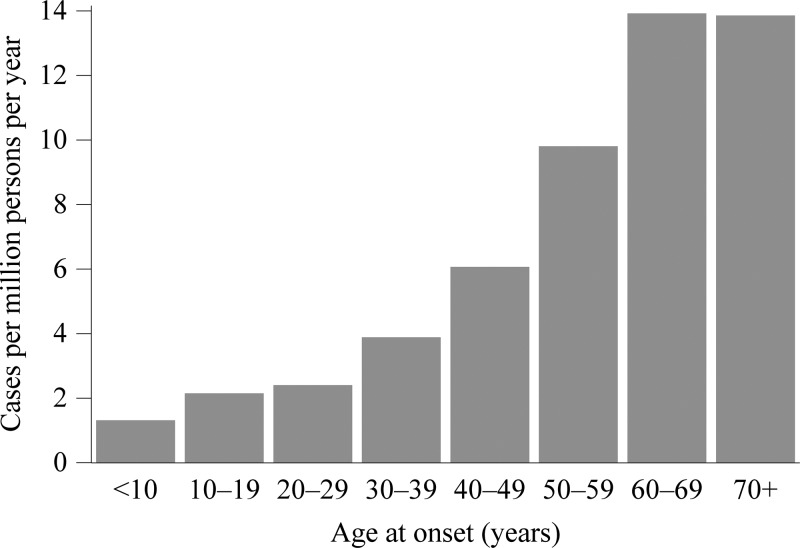
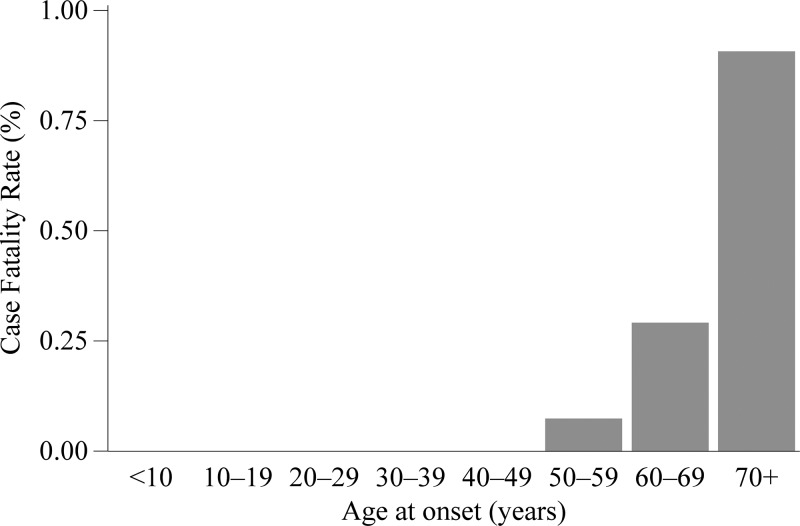
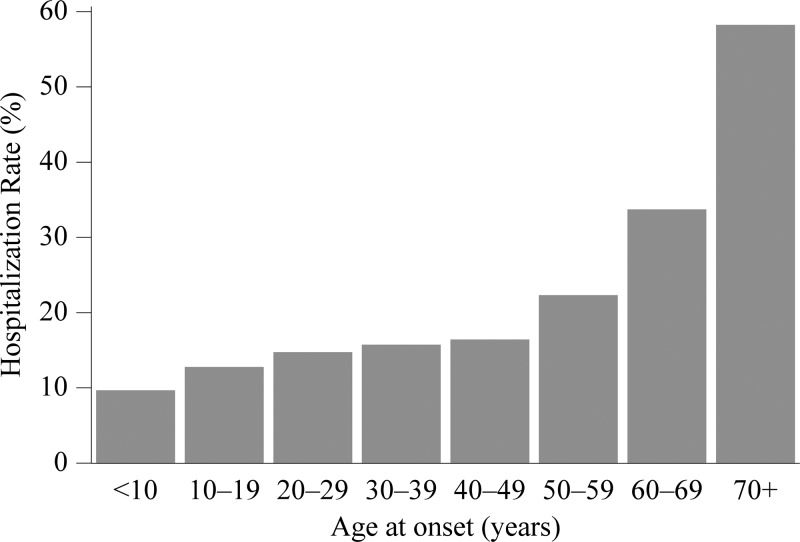
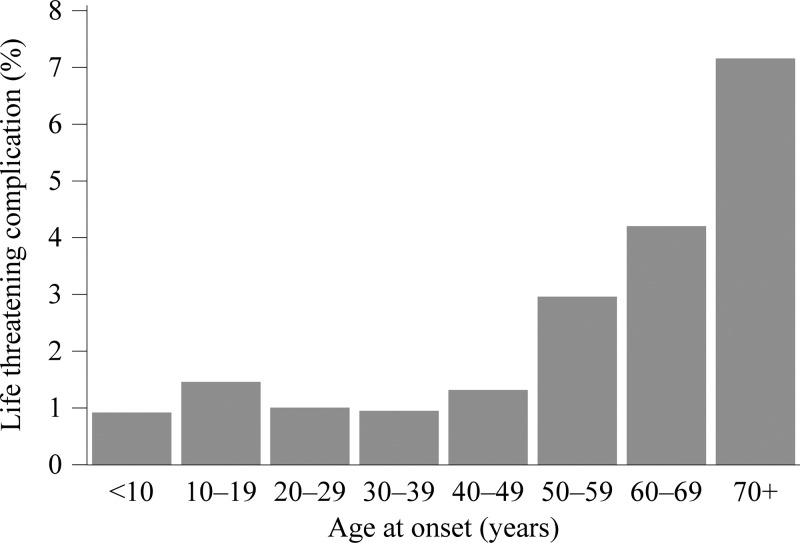
Human granulocytic anaplasmosis is an acute, febrile illness transmitted by the ticks Ixodes scapularis and Ixodes pacificus in the United States. We present a summary of passive surveillance data for cases of anaplasmosis with onset during 2008-2012. The overall reported incidence rate (IR) was 6.3 cases per million person-years. Cases were reported from 38 states and from New York City, with the highest incidence in Minnesota (IR = 97), Wisconsin (IR = 79), and Rhode Island (IR = 51). Thirty-seven percent of cases were classified as confirmed, almost exclusively by polymerase chain reaction. The reported case fatality rate was 0.3% and the reported hospitalization rate was 31%. IRs, hospitalization rates, life-threatening complications, and case fatality rates increased with age group. The IR increased from 2008 to 2012 and the geographic range of reported cases of anaplasmosis appears to have increased since 2000-2007. Our findings are consistent with previous case series and recent reports of the expanding range of the tick vector I. scapularis.
© The American Society of Tropical Medicine and Hygiene.
Figures
References
-
- Bakken JS, Dumler JS, Chen SM, Eckman MR, Vanetta LL, Walker DH. Human granulocytic ehrlichiosis in the Upper Midwest United States: a new species emerging? JAMA. 1994;272:212–218. - PubMed
-
- Centers for Disease Control and Prevention Human granulocytic ehrlichiosis—New York, 1995. MMWR Morb Mortal Wkly Rep. 1995;44:593–595. - PubMed
-
- Bakken JS, Krueth J, Wilson-Nordskog C, Tilden RL, Asanovich K, Dumler JS. Clinical and laboratory characteristics of human granulocytic ehrlichiosis. JAMA. 1996;275:199–205. - PubMed
-
- Hardalo CJ, Quagliarello V, Dumler JS. Human granulocytic ehrlichiosis in Connecticut: report of a fatal case. Clin Infect Dis. 1995;21:910–914. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
