

Combination therapy reduces the incidence of no-reflow after primary per-cutaneous coronary intervention in patients with ST-segment elevation acute myocardial infarction
- PMID: 25870616
- PMCID: PMC4394328
- DOI: 10.11909/j.issn.1671-5411.2015.02.003
Combination therapy reduces the incidence of no-reflow after primary per-cutaneous coronary intervention in patients with ST-segment elevation acute myocardial infarction
Abstract
Background: No-reflow is associated with an adverse outcome and higher mortality in patients with ST-segment elevation acute myocardial infarction (STEMI) who undergo percutaneous coronary intervention (PCI) and is considered a dynamic process characterized by multiple pathogenetic components. The aim of this study was to investigate the effectiveness of a combination therapy for the prevention of no-reflow in patient with acute myocardial infarction (AMI) undergoing primary PCI.
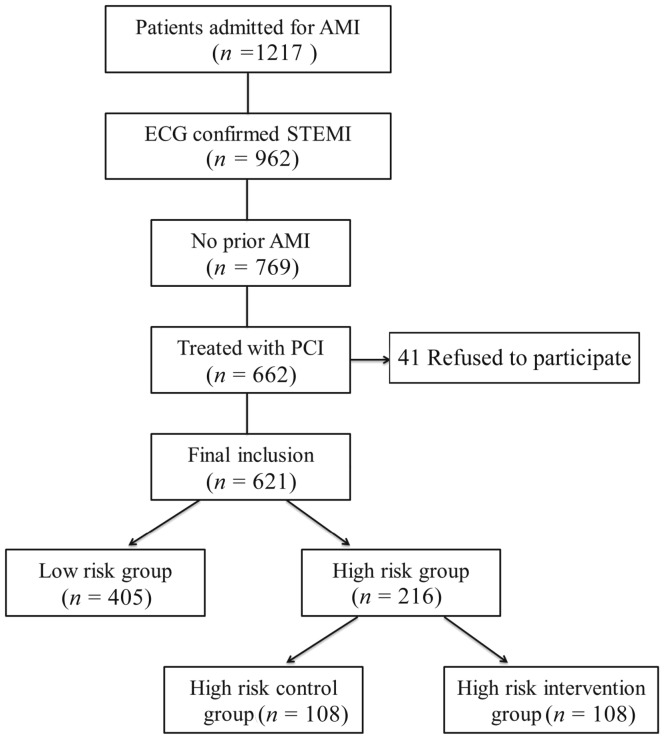
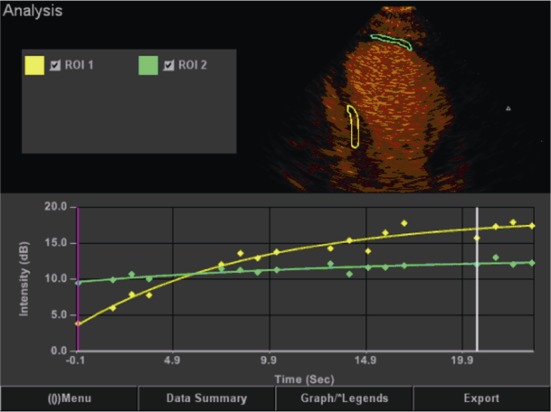
Methods: A total of 621 patients with STEMI who underwent emergency primary PCI were enrolled in this study. Patients with high risk of no-reflow (no-flow score ≥ 10, by using a no-flow risk prediction model, n = 216) were randomly divided into a controlled group (n = 108) and a combination therapy group (n = 108). Patients in the controlled group received conventional treatment, while patients in combination therapy group received high-dose (80 mg) atorvastatin pre-treatment, intracoronary administration of adenosine (140 µg/min per kilogram) during PCI procedure, platelet membrane glycoprotein IIb/IIIa receptor antagonist (tirofiban, 10µg/kg bolus followed by 0.15 µg/kg per minute) and thrombus aspiration. Myocardial contrast echocardiography was performed to assess the myocardial perfusion 72 h after PCI. Major adverse cardiac events (MACE) were followed up for six months.
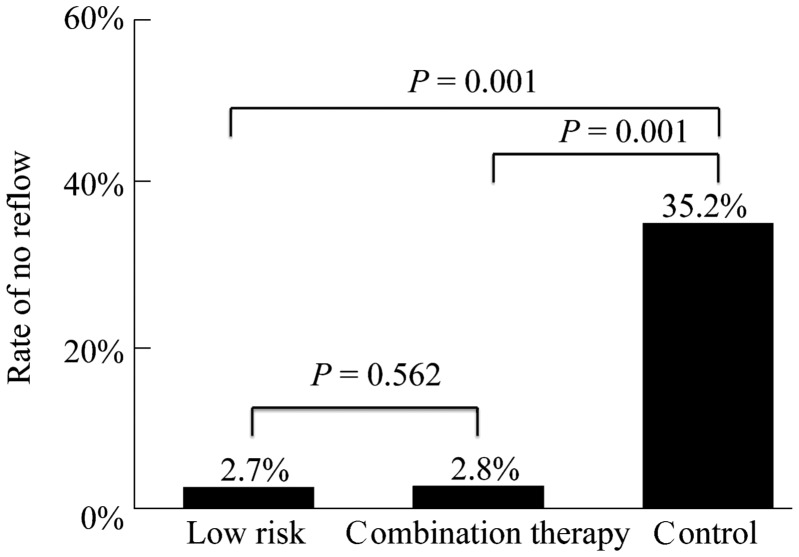
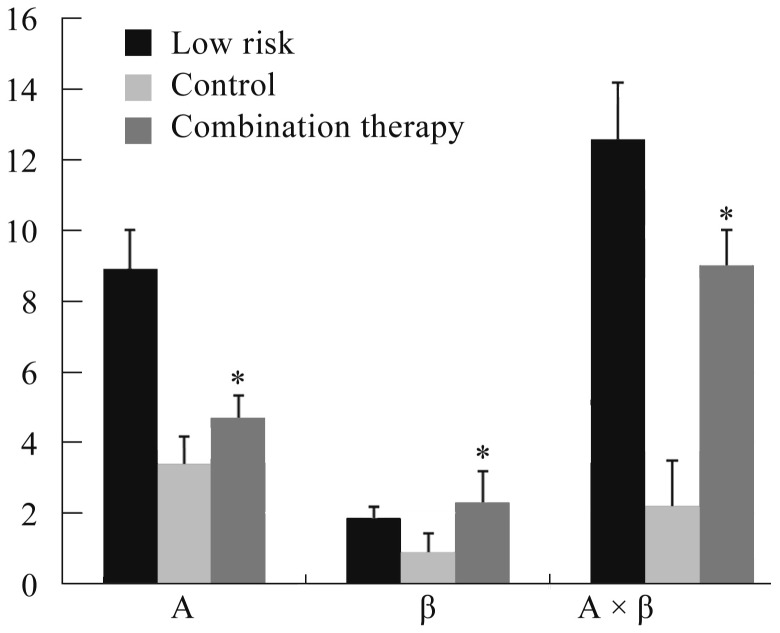
Results: Incidence of no-reflow in combination therapy group was 2.8%, which was similar to that in low risk group 2.7% and was significantly lower than that in control group (35.2%, P < 0.01). The myocardial perfusion (A × β) values were higher in combination therapy group than that in control group 72 h after PCI. After 6 months, there were six (6.3%) MACE events (one death, two non-fatal MIs and three revascularizations) in combination therapy group and 12 (13.2%) (four deaths, three non-fatal MIs and five revascularizations, P < 0.05) in control group.
Conclusions: Combination of thrombus aspiration, high-dose statin pre-treatment, intracoronary administration of adenosine during PCI procedure and platelet membrane glycoprotein IIb/IIIa receptor antagonist reduce the incidence of no-reflow after primary PCI in patients with acute myocardial infarction who are at high risk of no-reflow.
Keywords: Acute myocardial infarction; Myocardial contrast echocardiography; No-reflow phenomenon; Percutaneous coronary intervention; ST-elevation myocardial infarction.
Figures
Similar articles
-
Early Administration of Intracoronary Nitroprusside Compared with Thrombus Aspiration in Myocardial Perfusion for Acute Myocardial Infarction: A 3-Year Clinical Follow-Up Study.Acta Cardiol Sin. 2015 Sep;31(5):373-80. doi: 10.6515/acs20150515a. Acta Cardiol Sin. 2015. PMID: 27122896 Free PMC article.
-
Predictive value of admission red cell distribution width-platelet ratio for no-reflow phenomenon in acute ST segment elevation myocardial infarction undergoing primary percutaneous coronary intervention.Cardiol J. 2016;23(1):84-92. doi: 10.5603/CJ.a2015.0070. Epub 2015 Oct 27. Cardiol J. 2016. PMID: 26503078
-
Intracoronary fixed dose of nitroprusside via thrombus aspiration catheter for the prevention of the no-reflow phenomenon following primary percutaneous coronary intervention in acute myocardial infarction.Exp Ther Med. 2013 Aug;6(2):479-484. doi: 10.3892/etm.2013.1139. Epub 2013 Jun 4. Exp Ther Med. 2013. PMID: 24137212 Free PMC article.
-
Is Atherothromboaspiration a Possible Solution for the Prevention of No-Reflow Phenomenon in Acute Coronary Syndromes? Single Centre Experience and Review of the Literature.Curr Vasc Pharmacol. 2019;17(2):164-179. doi: 10.2174/1570161116666180101150956. Curr Vasc Pharmacol. 2019. PMID: 29298651 Review.
-
Emergency percutaneous coronary intervention (PCI) for the care of patients with ST-elevation myocardial infarction (STEMI).Minerva Cardioangiol. 2007 Oct;55(5):593-623. Minerva Cardioangiol. 2007. PMID: 17912165 Review.
Cited by
-
Development of local clinical practice guidelines in the real world: an evolving scene in China.Heart Asia. 2017 Jun 16;9(2):e010903. doi: 10.1136/heartasia-2017-010903. eCollection 2017. Heart Asia. 2017. PMID: 29467835 Free PMC article. No abstract available.
-
Evaluation of related factors, prediction and treatment drugs of no-reflow phenomenon in patients with acute ST-segment elevation myocardial infarction after direct PCI.Exp Ther Med. 2018 Apr;15(4):3940-3946. doi: 10.3892/etm.2018.5900. Epub 2018 Feb 27. Exp Ther Med. 2018. PMID: 29563988 Free PMC article.
-
Consensus Document of the Italian Association of Hospital Cardiologists (ANMCO), Italian Society of Cardiology (SIC), Italian Association of Interventional Cardiology (SICI-GISE) and Italian Society of Cardiac Surgery (SICCH): clinical approach to pharmacologic pre-treatment for patients undergoing myocardial revascularization procedures.Eur Heart J Suppl. 2017 May;19(Suppl D):D151-D162. doi: 10.1093/eurheartj/sux010. Epub 2017 May 2. Eur Heart J Suppl. 2017. PMID: 28751841 Free PMC article.
-
Efficacy and Safety of Thrombectomy Combined with Intracoronary Administration of Tirofiban in ST-segment Elevation Myocardial Infarction (STEMI).Med Sci Monit. 2016 Jul 31;22:2699-705. doi: 10.12659/msm.896703. Med Sci Monit. 2016. PMID: 27475844 Free PMC article. Clinical Trial.
-
Sodium nitroprusside injection immediately before balloon inflation during percutaneous coronary intervention.World J Clin Cases. 2021 Dec 26;9(36):11248-11254. doi: 10.12998/wjcc.v9.i36.11248. World J Clin Cases. 2021. PMID: 35071555 Free PMC article.
References
-
- Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361:13–20. - PubMed
-
- Niccoli G, Burzotta F, Galiuto L, et al. Myocardial no-reflow in humans. J Am Coll Cardiol. 2009;54:281–292. - PubMed
-
- Rezkalla SH, Kloner RA. Coronary no-reflow phenomenon: From the experimental laboratory to the cardiac catheterization laboratory. Catheter Cardiovasc Interv. 2008;72:950–957. - PubMed
-
- Rezkalla SH, Kloner RA. Coronary no-reflow phenomenon: from the experimental laboratory to the cardiac catheterization laboratory. Catheter Cardiovasc Interv. 2008;72:950–957. - PubMed
-
- Brosh D, Assali AR, Mager A, et al. Effect of no-reflow during primary percutaneous coronary intervention for acute myocardial infarction on six-month mortality. Am J Cardiol. 2007;99:442–445. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous