

Sutureless aortic valve replacement: a systematic review and meta-analysis
- PMID: 25870805
- PMCID: PMC4384251
- DOI: 10.3978/j.issn.2225-319X.2014.06.01
Sutureless aortic valve replacement: a systematic review and meta-analysis
Abstract
Background: Sutureless aortic valve replacement (SU-AVR) has emerged as an innovative alternative for treatment of aortic stenosis. By avoiding the placement of sutures, this approach aims to reduce cross-clamp and cardiopulmonary bypass (CPB) duration and thereby improve surgical outcomes and facilitate a minimally invasive approach suitable for higher risk patients. The present systematic review and meta-analysis aims to assess the safety and efficacy of SU-AVR approach in the current literature.
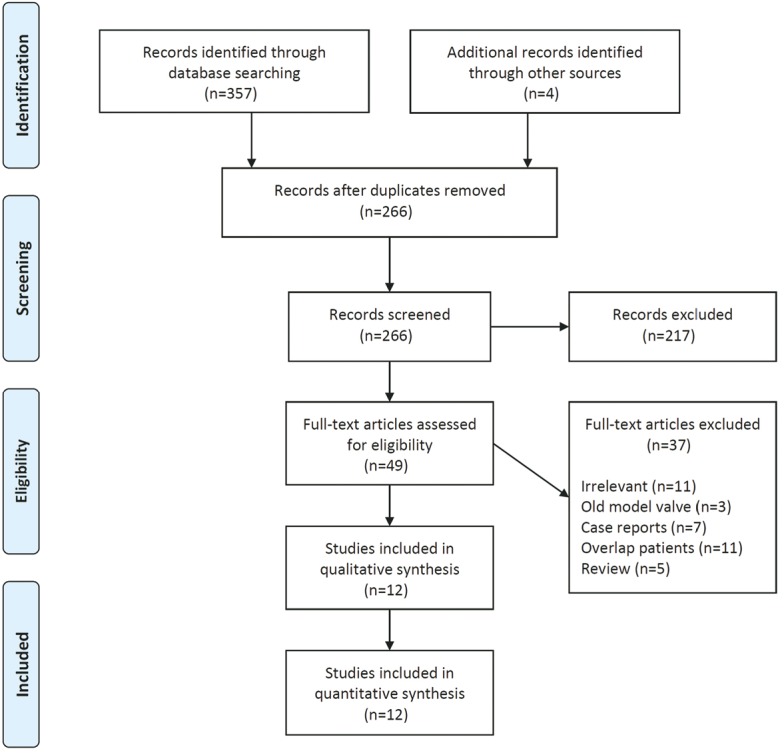
Methods: Electronic searches were performed using six databases from their inception to January 2014. Relevant studies utilizing sutureless valves for aortic valve implantation were identified. Data were extracted and analyzed according to predefined clinical endpoints.
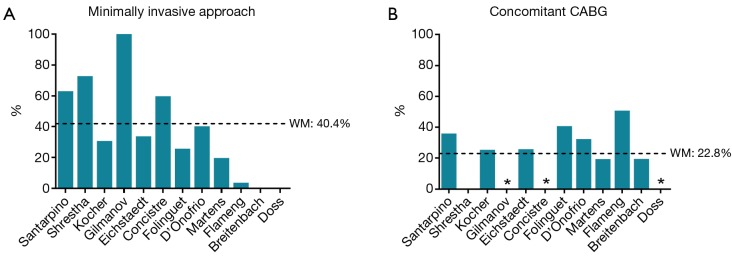
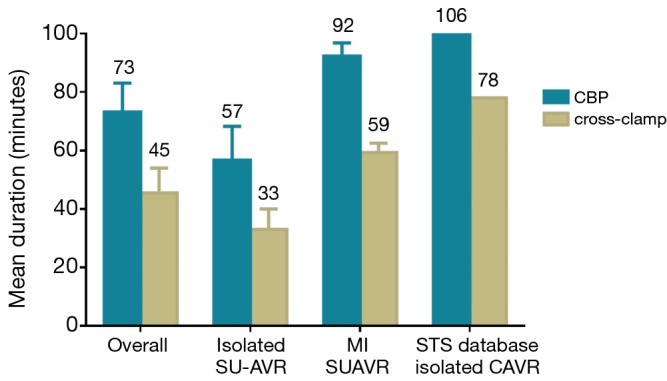
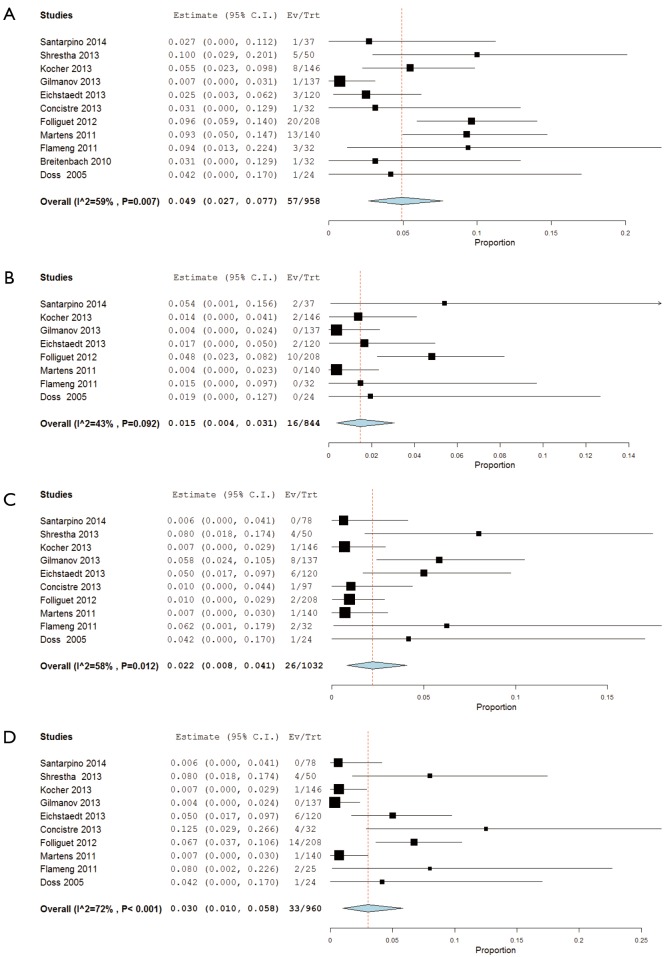
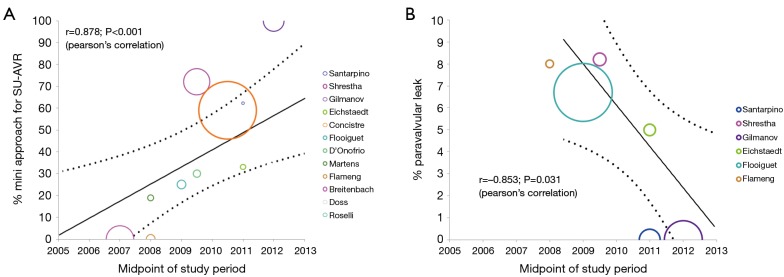
Results: Twelve studies were identified for inclusion of qualitative and quantitative analyses, all of which were observational reports. The minimally invasive approach was used in 40.4% of included patients, while 22.8% underwent concomitant coronary bypass surgery. Pooled cross-clamp and CPB duration for isolated AVR was 56.7 and 46.5 minutes, respectively. Pooled 30-day and 1-year mortality rates were 2.1% and 4.9%, respectively, while the incidences of strokes (1.5%), valve degenerations (0.4%) and paravalvular leaks (PVL) (3.0%) were acceptable.
Conclusions: The evaluation of current observational evidence suggests that sutureless aortic valve implantation is a safe procedure associated with shorter cross-clamp and CPB duration, and comparable complication rates to the conventional approach in the short-term.
Keywords: Sutureless; aortic valve replacement (AVR); meta-analysis; minimally invasive.
Figures
References
-
- Vahanian A, Otto CM. Risk stratification of patients with aortic stenosis. Eur Heart J 2010;31:416-23. - PubMed
-
- Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med 2010;363:1597-607. - PubMed
-
- Brown JM, O’Brien SM, Wu C, et al. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: changes in risks, valve types, and outcomes in the Society of Thoracic Surgeons National Database. J Thorac Cardiovasc Surg 2009;137:82-90. - PubMed
-
- Frilling B, von Renteln-Kruse W, Riess FC. Evaluation of operative risk in elderly patients undergoing aortic valve replacement: the predictive value of operative risk scores. Cardiology 2010;116:213-8. - PubMed
-
- Flameng W, Herregods MC, Hermans H, et al. Effect of sutureless implantation of the Perceval S aortic valve bioprosthesis on intraoperative and early postoperative outcomes. J Thorac Cardiovasc Surg 2011;142:1453-7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources