

Minimally invasive aortic valve replacement: 12-year single center experience
- PMID: 25870812
- PMCID: PMC4384246
- DOI: 10.3978/j.issn.2225-319X.2014.12.05
Minimally invasive aortic valve replacement: 12-year single center experience
Abstract
Background: This study reports the single center experience on minimally invasive aortic valve replacement (MIAVR), performed through a right anterior minithoracotomy or ministernotomy (MS).
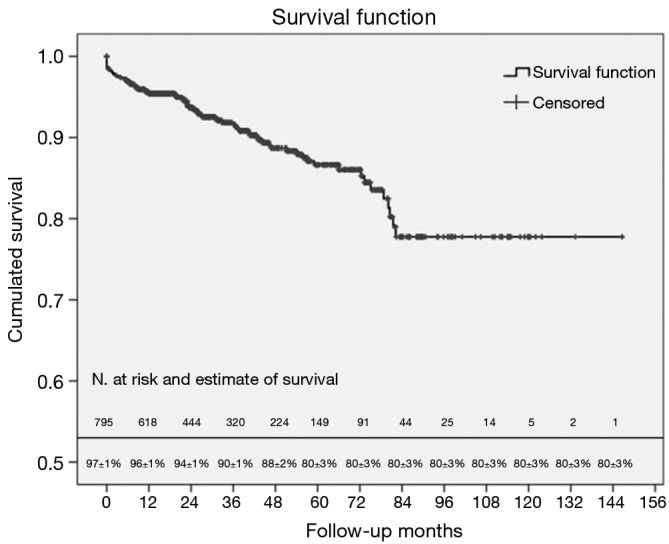
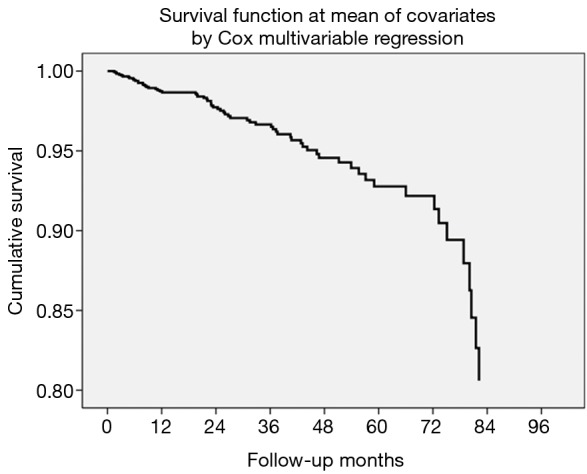
Methods: Eight hundred and fifty-three patients, who underwent MIAVR from 2002 to 2014, were retrospectively analyzed. Survival was evaluated using the Kaplan-Meier method. The Cox multivariable proportional hazards regression model was developed to identify independent predictors of follow-up mortality.
Results: Median age was 73.8, and 405 (47.5%) of patients were female. The overall 30-day mortality was 1.9%. Four hundred and forty-three (51.9%) and 368 (43.1%) patients received biological and sutureless prostheses, respectively. Median cardiopulmonary bypass time and aortic cross-clamping time were 108 and 75 minutes, respectively. Nineteen (2.2%) cases required conversion to full median sternotomy. Thirty-seven (4.3%) patients required re-exploration for bleeding. Perioperative stroke occurred in 15 (1.8%) patients, while transient ischemic attack occurred postoperative in 11 (1.3%). New onset atrial fibrillation was reported for 243 (28.5%) patients. After a median follow-up of 29.1 months (2,676.0 patient-years), survival rates at 1 and 5 years were 96%±1% and 80%±3%, respectively. Cox multivariable analysis showed that advanced age, history of cardiac arrhythmia, preoperative chronic renal failure, MS approach, prolonged mechanical ventilation and hospital stay as well as wound revision were associated with higher mortality.
Conclusions: MIAVR via both approaches is safe and feasible with excellent outcomes, and is associated with low conversion rate and low perioperative morbidity. Long term survival is at least comparable to that reported for conventional sternotomy AVR.
Keywords: Aortic valve replacement (AVR); heart valve prosthesis; minimally invasive heart surgery; outcomes.
Figures
References
-
- Nkomo VT, Gardin JM, Skelton TN, et al. Burden of valvular heart diseases: a population-based study. Lancet 2006;368:1005-11. - PubMed
-
- Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur Heart J 2003;24:1231-43. - PubMed
-
- Schmitto JD, Mokashi SA, Cohn LH. Minimally-invasive valve surgery. J Am Coll Cardiol 2010;56:455-62. - PubMed
-
- Johnston WF, Ailawadi G. Surgical management of minimally invasive aortic valve operations. Semin Cardiothorac Vasc Anesth 2012;16:41-51. - PubMed
LinkOut - more resources
Full Text Sources