

Mini-Bentall procedure
- PMID: 25870816
- PMCID: PMC4384256
- DOI: 10.3978/j.issn.2225-319X.2015.03.08
Mini-Bentall procedure
Abstract
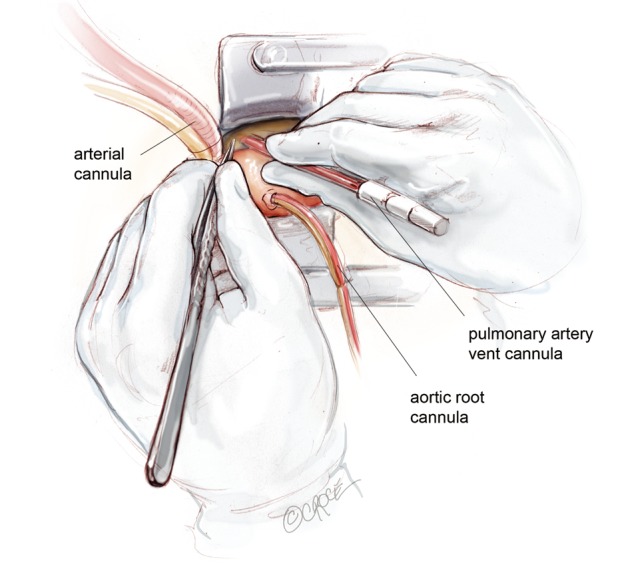
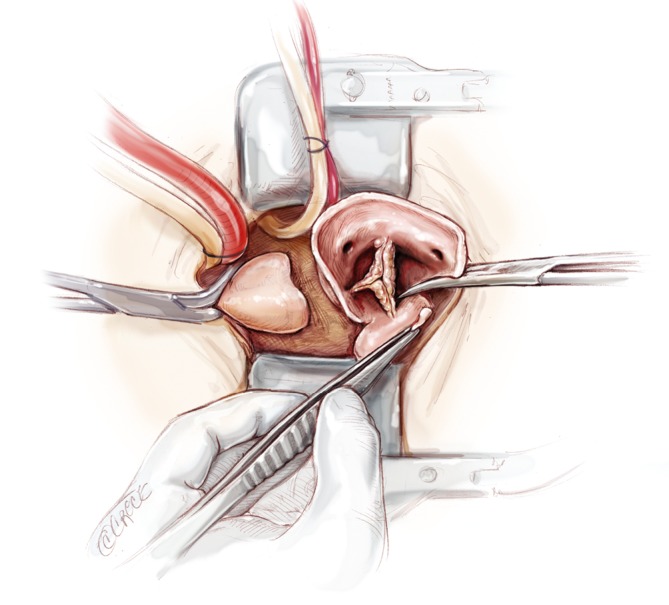
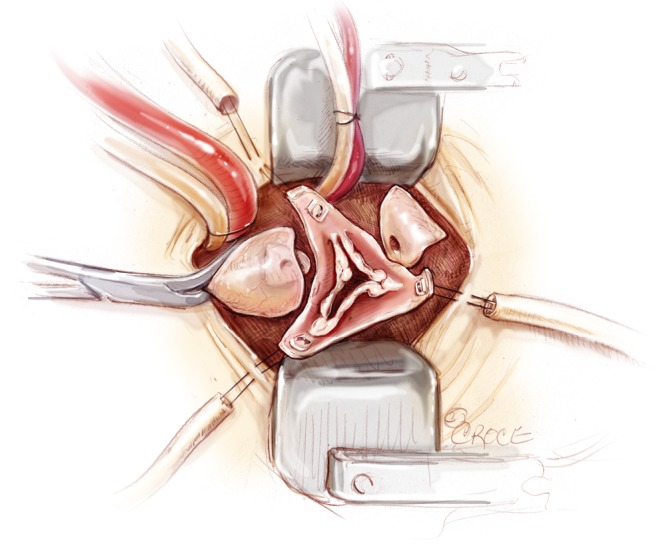
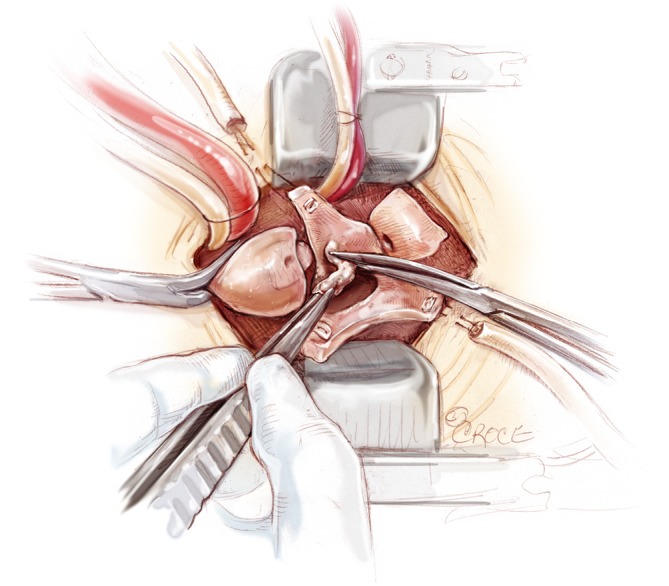
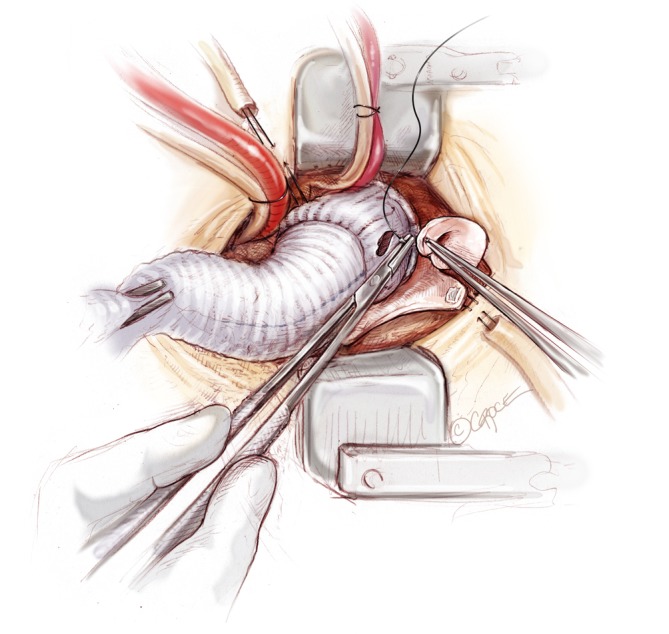
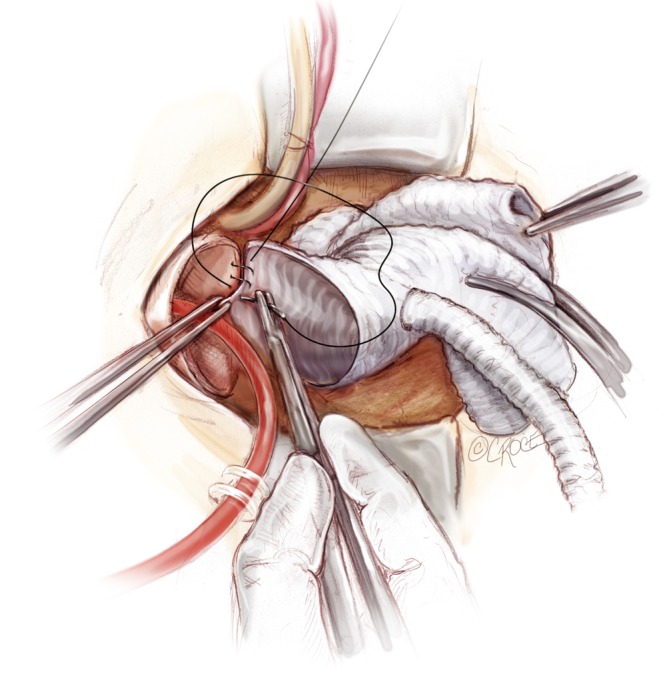
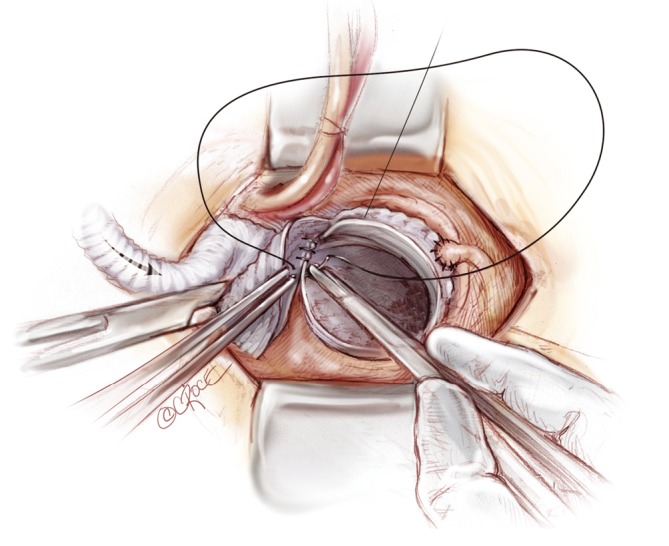
An important goal in cardiovascular and thoracic surgery is reducing surgical trauma to achieve faster recovery for our patients. Mini-Bentall procedure encompasses aortic root and ascending aortic replacement with re-implantation of coronary buttons, performed via a mini-sternotomy. The skin incision extends from the angle of Louis to the third intercostal space, usually measuring 5-7 cm in length. Through this incision, it is possible to perform isolated aortic root surgery and/or hemi-arch replacement. The present illustrated article describes the technical details on how I perform a Mini-Bentall procedure with hemi-arch replacement.
Keywords: Aortic root surgery; Bentall procedure; minimally invasive techniques.
Figures








References
Publication types
LinkOut - more resources
Full Text Sources