

Cost-effectiveness of first-line antiretroviral therapy for HIV-infected African children less than 3 years of age
- PMID: 25870982
- PMCID: PMC4536981
- DOI: 10.1097/QAD.0000000000000672
Cost-effectiveness of first-line antiretroviral therapy for HIV-infected African children less than 3 years of age
Abstract
Background: The International Maternal, Pediatric, and Adolescent Clinical Trials P1060 trial demonstrated superior outcomes for HIV-infected children less than 3 years old initiating antiretroviral therapy (ART) with lopinavir/ritonavir compared to nevirapine, but lopinavir/ritonavir is four-fold costlier.
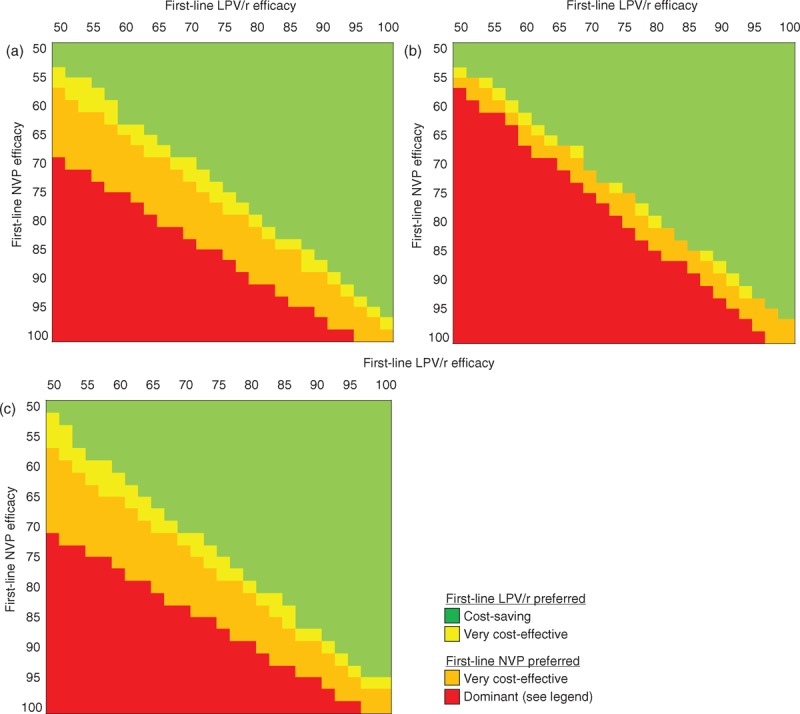
Design/methods: We used the Cost-Effectiveness of Preventing AIDS Complications (CEPAC)-Pediatric model, with published and P1060 data, to project outcomes under three strategies: no ART; first-line nevirapine (with second-line lopinavir/ritonavir); and first-line lopinavir/ritonavir (second-line nevirapine). The base-case examined South African children initiating ART at age 12 months; sensitivity analyses varied all key model parameters. Outcomes included life expectancy, lifetime costs, and incremental cost-effectiveness ratios [ICERs; dollars/year of life saved ($/YLS)]. We considered interventions with ICERs less than 1× per-capita gross domestic product (South Africa: $7500)/YLS as 'very cost-effective,' interventions with ICERs below 3× gross domestic product/YLS as 'cost-effective,' and interventions leading to longer life expectancy and lower lifetime costs as 'cost-saving'.
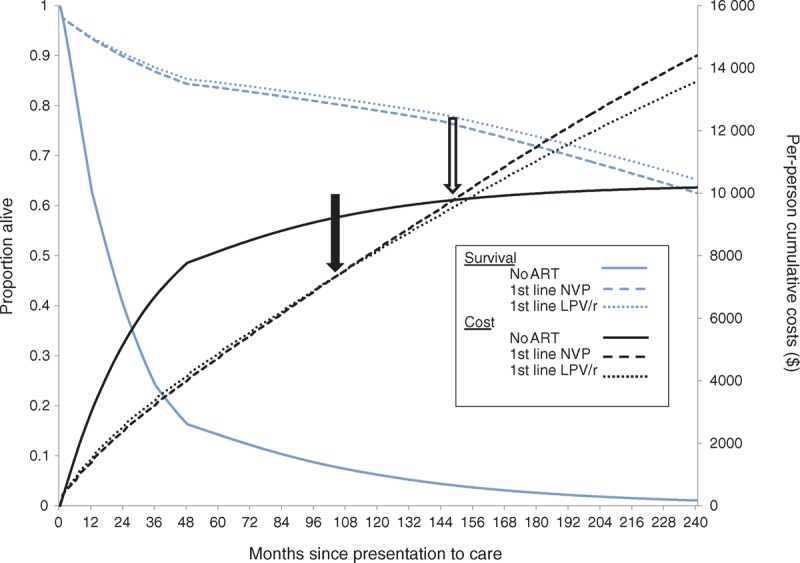
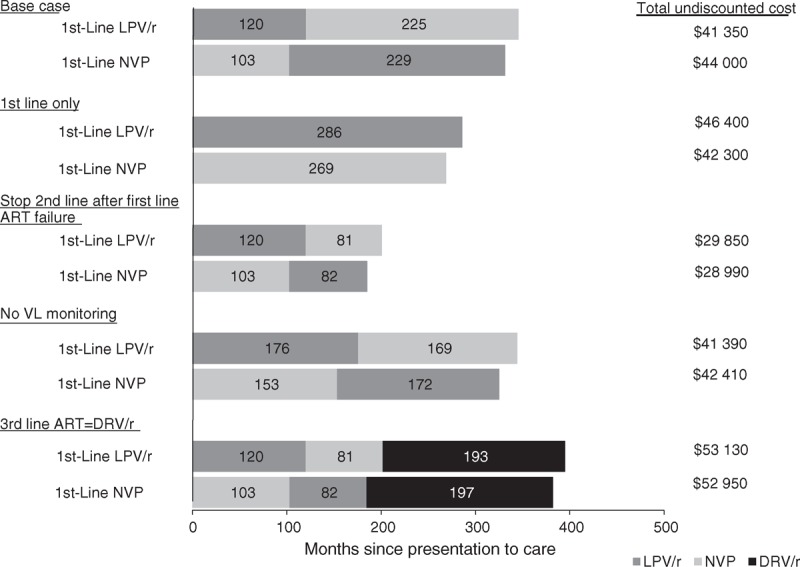
Results: Projected life expectancy was 2.8 years with no ART. Both ART regimens markedly improved life expectancy and were very cost-effective, compared to no ART. First-line lopinavir/ritonavir led to longer life expectancy (28.8 years) and lower lifetime costs ($41 350/person, from lower second-line costs) than first-line nevirapine (27.6 years, $44 030). First-line lopinavir/ritonavir remained cost-saving or very cost-effective compared to first-line nevirapine unless: liquid lopinavir/ritonavir led to two-fold higher virologic failure rates or 15-fold greater costs than in the base-case, or second-line ART following first-line lopinavir/ritonavir was very ineffective.
Conclusions: On the basis of P1060 data, first-line lopinavir/ritonavir leads to longer life expectancy and is cost-saving or very cost-effective compared to first-line nevirapine. This supports WHO guidelines, but increasing access to pediatric ART is critical regardless of the regimen used.
Figures
Comment in
-
First-line antiretroviral therapy for HIV-infected children.AIDS. 2015 Jun 19;29(10):1261-2. doi: 10.1097/QAD.0000000000000727. AIDS. 2015. PMID: 26035324 No abstract available.
References
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS). UNAIDS report on the global AIDS epidemic. 2013. http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiolo... [Accessed 20 November 2014]
-
- Newell ML, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F. Ghent International AIDS Society (IAS) Working Group on HIV Infection in Women and Children Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet 2004; 364:1236–1243. - PubMed
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS). Progress report on the global plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive, 2013. http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspubl... [Accessed 21 November 2014]
-
- UNICEF, UNAIDS. Towards an AIDS-free generation: children and AIDS sixth stocktaking report. 2013. http://www.childrenandaids.org/ [Accessed 19 November 2014]
-
- Sohn AH, Nuttall JJ, Zhang F. Sequencing of antiretroviral therapy in children in low- and middle-income countries. Curr Opin HIV AIDS 2010; 5:54–60. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UM1 AI068632/AI/NIAID NIH HHS/United States
- R01 HD079214/HD/NICHD NIH HHS/United States
- K24 AI062476/AI/NIAID NIH HHS/United States
- UM1AI068632/AI/NIAID NIH HHS/United States
- UM1 AI068616/AI/NIAID NIH HHS/United States
- K01 AI078754/AI/NIAID NIH HHS/United States
- UM1AI068616/AI/NIAID NIH HHS/United States
- R01 AI058736/AI/NIAID NIH HHS/United States
- 001/WHO_/World Health Organization/International
- U01AI09919/AI/NIAID NIH HHS/United States
- U01 AI069911/AI/NIAID NIH HHS/United States
- U01 AI069919/AI/NIAID NIH HHS/United States
- N01-DK-9-001/HHSN267200800001C/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
