

The characteristics of superficial siderosis and convexity subarachnoid hemorrhage and clinical relevance in suspected cerebral amyloid angiopathy
- PMID: 25871492
- PMCID: PMC4458203
- DOI: 10.1159/000381223
The characteristics of superficial siderosis and convexity subarachnoid hemorrhage and clinical relevance in suspected cerebral amyloid angiopathy
Abstract
Background and aims: Systematic studies of superficial siderosis (SS) and convexity subarachnoid hemorrhage (cSAH) in patients with suspected cerebral amyloid angiopathy (CAA) without lobar intracerebral hemorrhage (ICH) are lacking. We sought to determine the potential anatomic correlation between SS/cSAH and transient focal neurological episodes (TFNE) and whether SS/cSAH is predictor of future cerebral hemorrhagic events in these patients.
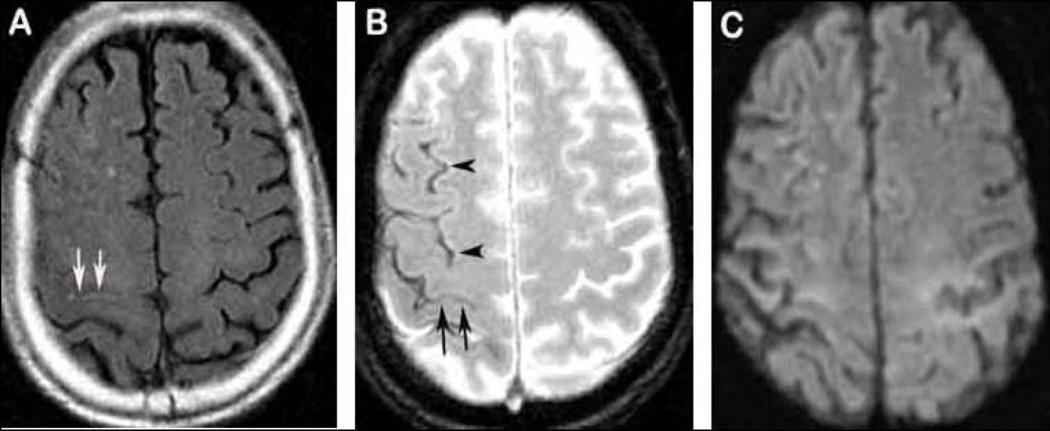
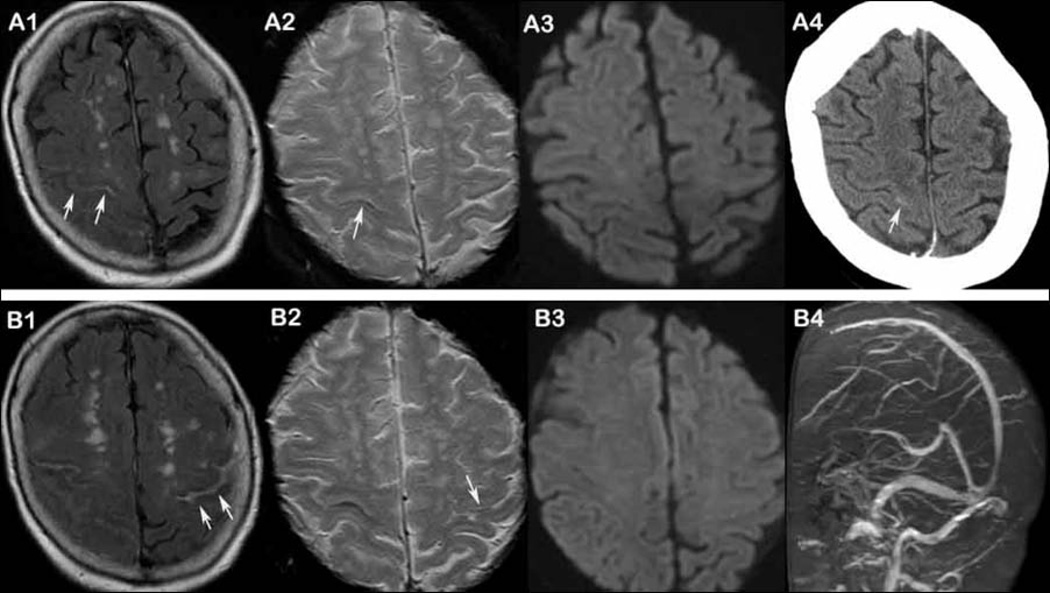
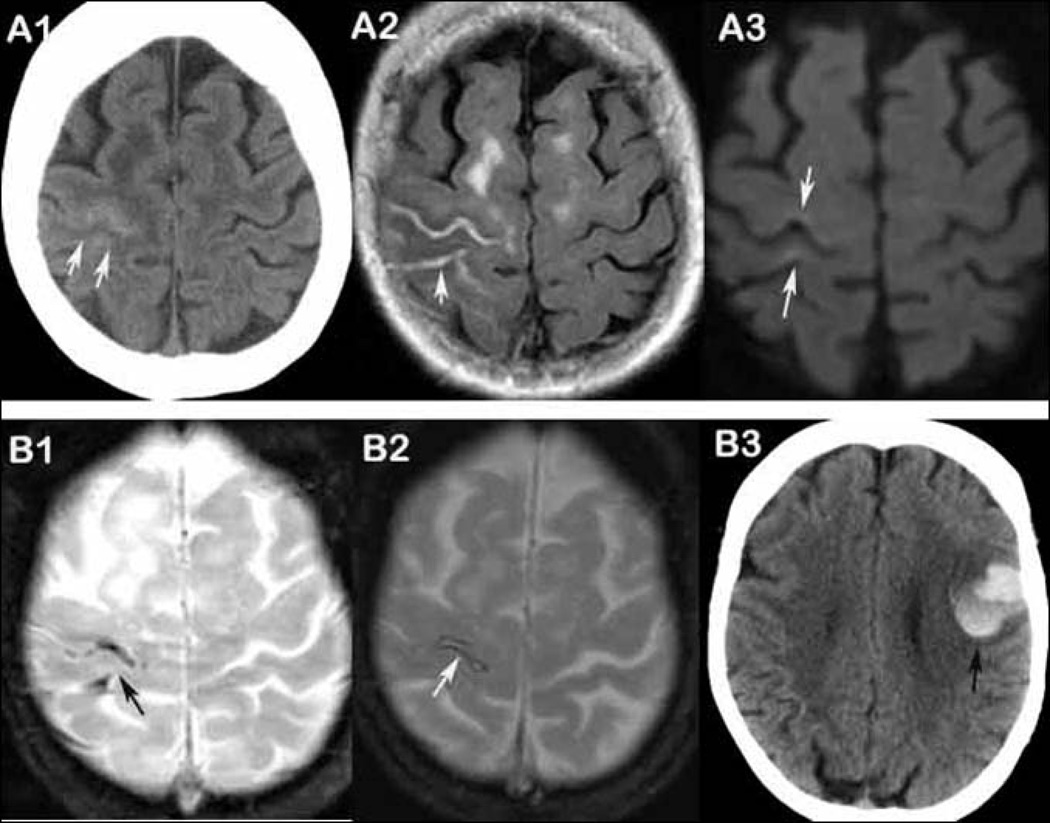
Methods: We enrolled 90 consecutive patients with suspected CAA (due to the presence of strictly lobar microbleeds (CMBs) and/or SS/cSAH) but without the history of symptomatic lobar ICH who underwent brain MRI including T2*-weighted, diffusion-weighted imaging and fluid-attenuated inversion recovery sequences from an ongoing single center CAA cohort from 1998 to 2012. Evaluation of SS, cSAH and CMBs was performed. Medical records and follow-up information were obtained from prospective databases and medical charts. TFNE was defined according to published criteria and electroencephalogram reports were reviewed.
Results: Forty-one patients (46%) presented with SS and/or cSAH. The prevalence of TFNE was significantly higher in those with SS/cSAH (61 vs. 10%; p < 0.001) and anatomically correlated with the location of cSAH, but not SS. The majority of TFNE in patients with SS/cSAH presented with spreading sensory symptoms. Intermittent focal slowing on electroencephalogram was present in the same area as SS/cSAH in 6 patients, but no epileptiform activity was found in any patients. Among those with available clinical follow-up (76/90 patients, 84%), ten patients with SS/cSAH (29%, median time from the scan for all patients with SS/cSAH: 21 months) had a symptomatic cerebral bleeding event on follow up (average time to events: 34 months) compared with only 1 event (2.4%, 25 months from the scan) in patients without SS/cSAH (time to event: 25 months) (p = 0.001). The location of hemorrhages on follow-up scan was not in the same location of previously noted SS/cSAH in 9 of 10 patients. Follow-up imaging was obtained in 9 of 17 patients with cSAH and showed evidence of SS in the same location as initial cSAH in all these 9 cases.
Conclusions: SS/cSAH is common in patients with suspected CAA without lobar intracerebral hemorrhage and may have a significantly higher risk of future cerebral bleeding events, regardless of the severity of the baseline CMB burden. The findings further highlight a precise anatomical correlation between TFNE and cSAH, but not SS. Distinct from transient ischemic attack or seizure, the majority of TFNE caused by SS/cSAH appear to present with spreading sensory symptoms.
© 2015 S. Karger AG, Basel.
Figures
References
-
- Charidimou A, Gang Q, Werring DJ. Sporadic cerebral amyloid angiopathy revisited: recent insights into pathophysiology and clinical spectrum. Journal of neurology, neurosurgery, and psychiatry. 2012;83:124–137. - PubMed
-
- Greenberg SM, Eng JA, Ning M, Smith EE, Rosand J. Hemorrhage burden predicts recurrent intracerebral hemorrhage after lobar hemorrhage. Stroke. 2004;35:1415–1420. - PubMed
-
- Greenberg SM, O'Donnell HC, Schaefer PW, Kraft E. MRI detection of new hemorrhages: potential marker of progression in cerebral amyloid angiopathy. Neurology. 1999;53:1135–1138. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
