

The renal protective effect of angiotensin receptor blockers depends on intra-individual response variation in multiple risk markers
- PMID: 25872610
- PMCID: PMC4594704
- DOI: 10.1111/bcp.12655
The renal protective effect of angiotensin receptor blockers depends on intra-individual response variation in multiple risk markers
Abstract
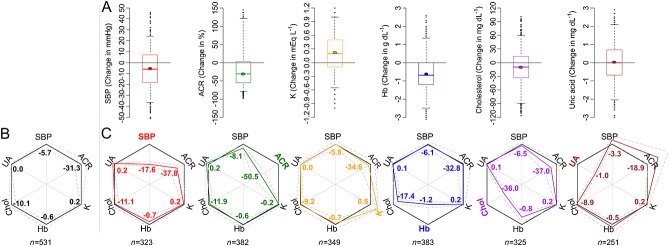
Aims: Angiotensin receptor blockers (ARBs) are renoprotective and targeted to blood pressure. However, ARBs have multiple other (off-target) effects which may affect renal outcome. It is unknown whether on-target and off-target effects are congruent within individuals. If not, this variation in short term effects may have important implications for the prediction of individual long term renal outcomes. Our aim was to assess intra-individual variability in multiple parameters in response to ARBs in type 2 diabetes.
Methods: Changes in systolic blood pressure (SBP), albuminuria, potassium, haemoglobin, cholesterol and uric acid after 6 months of losartan treatment were assessed in the RENAAL database. Improvement in predictive performance of renal outcomes (ESRD or doubling serum creatinine) for each individual using ARB-induced changes in all risk markers was assessed by the relative integrative discrimination index (RIDI).
Results: SBP response showed high variability (mean -5.7 mmHg, 5(th) to 95(th) percentile -36.5 to +24.0 mmHg) between individuals. Changes in off-target parameters also showed high variability between individuals. No congruency was observed between responses to losartan in multiple parameters within individuals. Using individual responses in all risk markers significantly improved renal risk prediction (RIDI 30.4%, P < 0.01) compared with using only SBP changes. Results were successfully replicated in two independent trials with irbesartan, IDNT and IRMA-2.
Conclusions: In this post hoc analysis we showed that ARBs have multiple off-target effects which vary between and within individuals. Combining all ARB-induced responses beyond SBP provides a more accurate prediction of who will benefit from ARB therapy. Prospective trials are required to validate these findings.
Keywords: angiotensin receptor blockers; personalized medicine; renal disease; type 2 diabetes.
© 2015 The British Pharmacological Society.
Figures
References
-
- Volpe M, Cosentino F, Tocci G, Palano F, Paneni F. Antihypertensive therapy in diabetes: The legacy effect and RAAS blockade. Curr Hypertens Rep. 2011;13:318–24. - PubMed
-
- Steckelings UM, Rompe F, Kaschina E, Unger T. The evolving story of the RAAS in hypertension, diabetes and CV disease ? moving from macrovascular to microvascular targets. Fundam Clin Pharmacol. 2009;23:693–703. - PubMed
-
- Smink PA, Bakker SJL, Laverman GD, Berl T, Cooper ME, de Zeeuw D, Lambers Heerspink HJ. An initial reduction in serum uric acid during angiotensin receptor blocker treatment is associated with cardiovascular protection: A post-hoc analysis of the RENAAL and IDNT trials. J Hypertens. 2012;30:1022–8. - PubMed
-
- Miao Y, Dobre D, Lambers Heerspink HJ, Brenner BM, Cooper ME, Parving H, Shahinfar S, Grobbee D, Zeeuw D. Increased serum potassium affects renal outcomes: A post hoc analysis of the reduction of endpoints in NIDDM with the angiotensin II antagonist losartan (RENAAL) trial. Diabetologia. 2011;54:44–50. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
