

Persistent Occiput Posterior position - OUTcomes following manual rotation (POP-OUT): study protocol for a randomised controlled trial
- PMID: 25872776
- PMCID: PMC4436169
- DOI: 10.1186/s13063-015-0603-7
Persistent Occiput Posterior position - OUTcomes following manual rotation (POP-OUT): study protocol for a randomised controlled trial
Abstract
Background: Occiput posterior position is the most common malpresentation in labour, contributes to about 18% of emergency caesarean sections and is associated with a high risk of assisted delivery. Caesarean section is now a major contributing factor to maternal mortality and morbidity following childbirth in developed countries. Obstetric intervention by forceps and ventouse delivery is associated with complications to the maternal genital tract and to the neonate, respectively. There is level 2 evidence that prophylactic manual rotation reduces the caesarean section rate and assisted vaginal delivery. But there has been no adequately powered randomised controlled trial. This is a protocol for a double-blinded, multicentre, randomised controlled clinical trial to define whether this intervention decreases the operative delivery (caesarean section, forceps or vacuum delivery) rate.
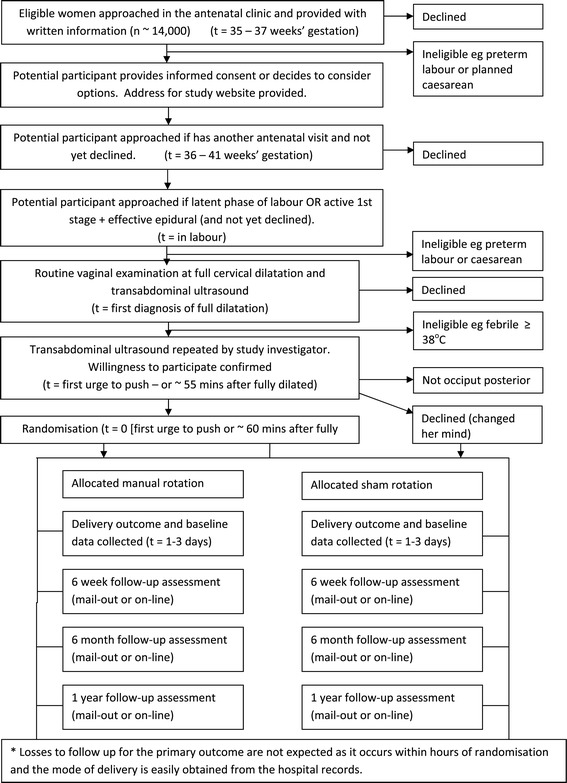
Methods/design: Eligible participants will be (greater than or equal to) 37 weeks' with a singleton pregnancy and a cephalic presentation in the occiput posterior position on transabdominal ultrasound early in the second stage of labour. Based on a background risk of operative delivery of 68%, then for a reduction to 50%, an alpha value of 0.05 and a beta value of 0.2, 254 participants will need to be enrolled. This study has been approved by the Ethics Review Committee (RPAH Zone) of the Sydney Local Health District, Sydney, Australia, and protocol number X110410. Participants with written consent will be randomised to either prophylactic manual rotation or a sham procedure. The primary outcome will be operative delivery (defined as vacuum, forceps and/or caesarean section deliveries). Secondary outcomes will be caesarean section, significant maternal mortality/morbidity and significant perinatal mortality/morbidity. Analysis will be by intention-to-treat. Primary and secondary outcomes will be compared using a chi-squared test. A logistic regression for the primary outcome will be undertaken to account for potential confounders. The results of the trial will be presented at one or more medical conferences. The trial will be submitted to peer review journals for consideration for publication. There will be potential to incorporate the results into professional guidelines for obstetricians and midwives.
Trial registration: The Australian New Zealand Clinical Trials Registry ACTRN12612001312831 . Trial registered 12 December 2012.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
