

Efficacy and oncologic safety of nerve-sparing radical hysterectomy for cervical cancer: a randomized controlled trial
- PMID: 25872890
- PMCID: PMC4397238
- DOI: 10.3802/jgo.2015.26.2.90
Efficacy and oncologic safety of nerve-sparing radical hysterectomy for cervical cancer: a randomized controlled trial
Abstract
Objective: A prospective, randomized controlled trial was conducted to evaluate the efficacy of nerve-sparing radical hysterectomy (NSRH) in preserving bladder function and its oncologic safety in the treatment of cervical cancer.
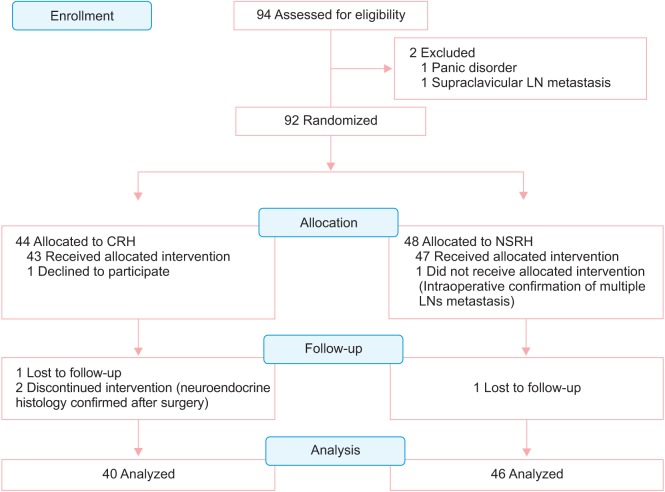
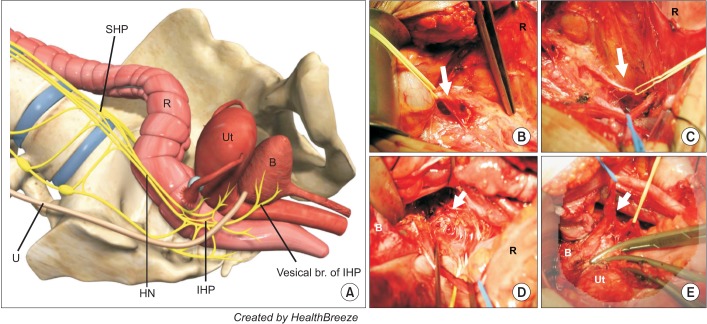
Methods: From March 2003 to November 2005, 92 patients with cervical cancer stage IA2 to IIA were randomly assigned for surgical treatment with conventional radical hysterectomy (CRH) or NSRH, and 86 patients finally included in the analysis. Adequacy of nerve sparing, radicality, bladder function, and oncologic safety were assessed by quantifying the nerve fibers in the paracervix, measuring the extent of paracervix and harvested lymph nodes (LNs), urodynamic study (UDS) with International Prostate Symptom Score (IPSS), and 10-year disease-free survival (DFS), respectively.
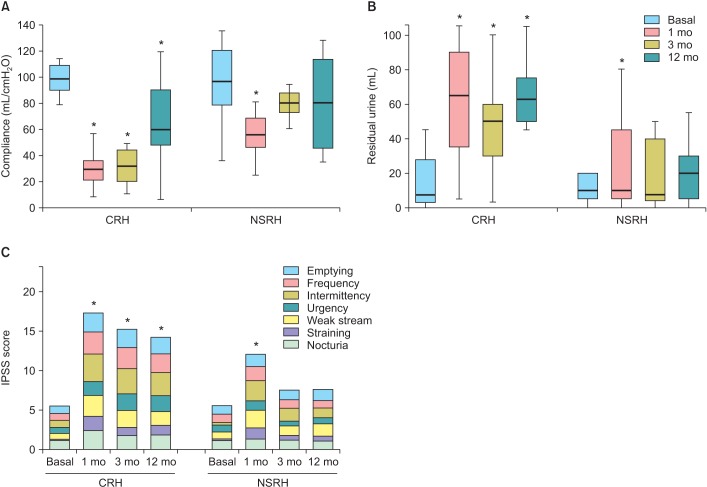
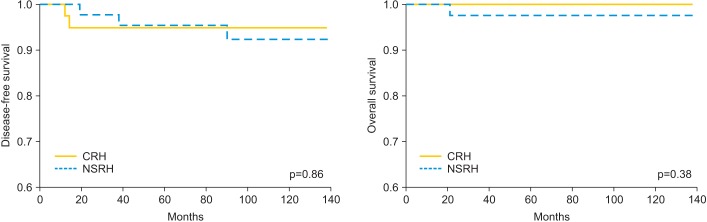
Results: There were no differences in clinicopathologic characteristics between two groups. The median number of nerve fiber was 12 (range, 6 to 21) and 30 (range, 17 to 45) in the NSRH and CRH, respectively (p<0.001). The extent of resected paracervix and number of LNs were not different between the two groups. Volume of residual urine and bladder compliance were significantly deteriorated at 12 months after CRH. On the contrary, all parameters of UDS were recovered no later than 3 months after NSRH. Evaluation of the IPSS showed that the frequency of long-term urinary symptom was higher in CRH than in the NSRH group. The median duration before the postvoid residual urine volume became less than 50 mL was 11 days (range, 7 to 26 days) in NSRH group and was 18 days (range, 10 to 85 days) in CRH group (p<0.001). No significant difference was observed in the 10-year DFS between two groups.
Conclusion: NSRH appears to be effective in preserving bladder function without sacrificing oncologic safety.
Keywords: Disease-Free Survival; Hysterectomy; Urinary Bladder, Neurogenic; Uterine Cervical Neoplasms.
Conflict of interest statement
Figures
Comment in
-
Nerve-sparing radical hysterectomy: time for a new standard of care for cervical cancer?J Gynecol Oncol. 2015 Apr;26(2):81-2. doi: 10.3802/jgo.2015.26.2.81. J Gynecol Oncol. 2015. PMID: 25872887 Free PMC article. No abstract available.
References
-
- Donato DM. Surgical management of stage IB-IIA cervical carcinoma. Semin Surg Oncol. 1999;16:232–235. - PubMed
-
- Zullo MA, Manci N, Angioli R, Muzii L, Panici PB. Vesical dysfunctions after radical hysterectomy for cervical cancer: a critical review. Crit Rev Oncol Hematol. 2003;48:287–293. - PubMed
-
- Ercoli A, Delmas V, Gadonneix P, Fanfani F, Villet R, Paparella P, et al. Classical and nerve-sparing radical hysterectomy: an evaluation of the risk of injury to the autonomous pelvic nerves. Surg Radiol Anat. 2003;25:200–206. - PubMed
-
- Maas CP, Trimbos JB, DeRuiter MC, van de Velde CJ, Kenter GG. Nerve sparing radical hysterectomy: latest developments and historical perspective. Crit Rev Oncol Hematol. 2003;48:271–279. - PubMed
-
- Landoni F, Maneo A, Cormio G, Perego P, Milani R, Caruso O, et al. Class II versus class III radical hysterectomy in stage IB-IIA cervical cancer: a prospective randomized study. Gynecol Oncol. 2001;80:3–12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
