

Conventional versus nerve-sparing radical surgery for cervical cancer: a meta-analysis
- PMID: 25872891
- PMCID: PMC4397225
- DOI: 10.3802/jgo.2015.26.2.100
Conventional versus nerve-sparing radical surgery for cervical cancer: a meta-analysis
Abstract
Objective: Although nerve-sparing radical surgery (NSRS) is an emerging technique for reducing surgery-related dysfunctions, its efficacy is controversial in patients with cervical cancer. Thus, we performed a meta-analysis to compare clinical outcomes, and urinary, anorectal, and sexual dysfunctions between conventional radical surgery (CRS) and NSRS.
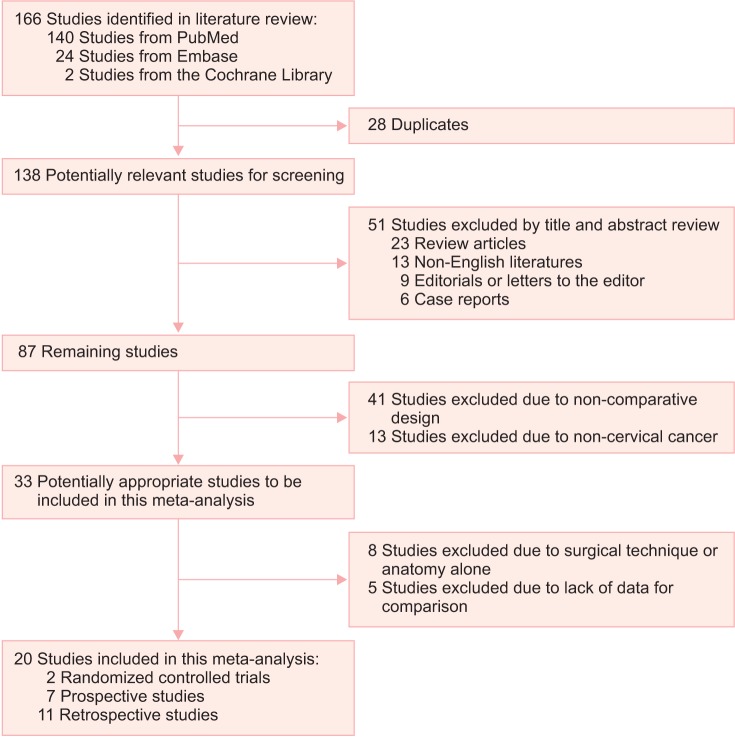
Methods: After searching PubMed, Embase, and the Cochrane Library, two randomized controlled trials, seven prospective and eleven retrospective cohort studies were included with 2,253 patients from January 2000 to February 2014. We performed crude analyses and then conducted subgroup analyses according to study design, quality of study, surgical approach, radicality, and adjustment for potential confounding factors.
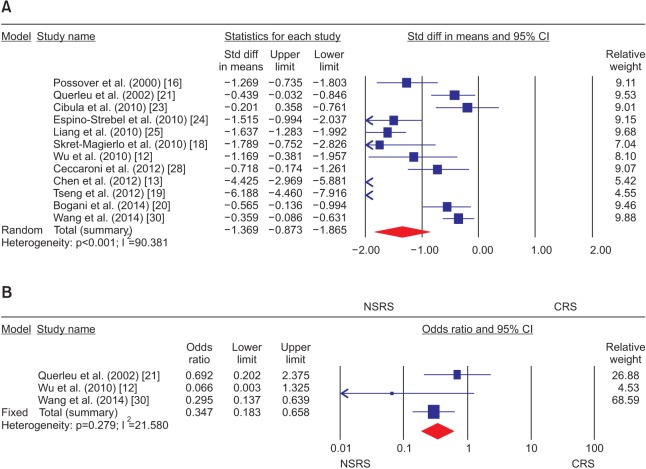
Results: Crude analyses showed decreases in blood loss, hospital stay, frequency of intraoperative complications, length of the resected vagina, duration of postoperative catheterization (DPC), urinary frequency, and abnormal sensation in NSRS, whereas there were no significant differences in other clinical parameters and dysfunctions between CRS and NSRS. In subgroup analyses, operative time was longer (standardized difference in means, 0.948; 95% confidence interval [CI], 0.642 to 1.253), while intraoperative complications were less common (odds ratio, 0.147; 95% CI, 0.035 to 0.621) in NSRS. Furthermore, subgroup analyses showed that DPC was shorter, urinary incontinence or frequency, and constipation were less frequent in NSRS without adverse effects on survival and sexual functions.
Conclusion: NSRS may not affect prognosis and sexual dysfunctions in patients with cervical cancer, whereas it may decrease intraoperative complications, and urinary and anorectal dysfunctions despite long operative time and short length of the resected vagina when compared with CRS.
Keywords: Hysterectomy; Intraoperative Complications; Meta-Analysis; Radical Surgery; Urinary Retention; Uterine Cervical Neoplasms.
Conflict of interest statement
Figures

Comment in
-
Nerve-sparing radical hysterectomy: time for a new standard of care for cervical cancer?J Gynecol Oncol. 2015 Apr;26(2):81-2. doi: 10.3802/jgo.2015.26.2.81. J Gynecol Oncol. 2015. PMID: 25872887 Free PMC article. No abstract available.
References
-
- Ditto A, Martinelli F, Borreani C, Kusamura S, Hanozet F, Brunelli C, et al. Quality of life and sexual, bladder, and intestinal dysfunctions after class III nerve-sparing and class II radical hysterectomies: a questionnaire-based study. Int J Gynecol Cancer. 2009;19:953–957. - PubMed
-
- Kim HS, Choi CH, Lim MC, Chang SJ, Kim YB, Kim MA, et al. Safe criteria for less radical trachelectomy in patients with early-stage cervical cancer: a multicenter clinicopathologic study. Ann Surg Oncol. 2012;19:1973–1979. - PubMed
-
- Zullo MA, Manci N, Angioli R, Muzii L, Panici PB. Vesical dysfunctions after radical hysterectomy for cervical cancer: a critical review. Crit Rev Oncol Hematol. 2003;48:287–293. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
