

Association between exposure to nonactionable physiologic monitor alarms and response time in a children's hospital
- PMID: 25873486
- PMCID: PMC4456276
- DOI: 10.1002/jhm.2331
Association between exposure to nonactionable physiologic monitor alarms and response time in a children's hospital
Abstract
Background: Alarm fatigue is reported to be a major threat to patient safety, yet little empirical data support its existence in the hospital.
Objective: To determine if nurses exposed to high rates of nonactionable physiologic monitor alarms respond more slowly to subsequent alarms that could represent life-threatening conditions.
Design: Observational study using video.
Setting: Freestanding children's hospital.
Patients: Pediatric intensive care unit (PICU) patients requiring inotropic support and/or mechanical ventilation, and medical ward patients.
Intervention: None.
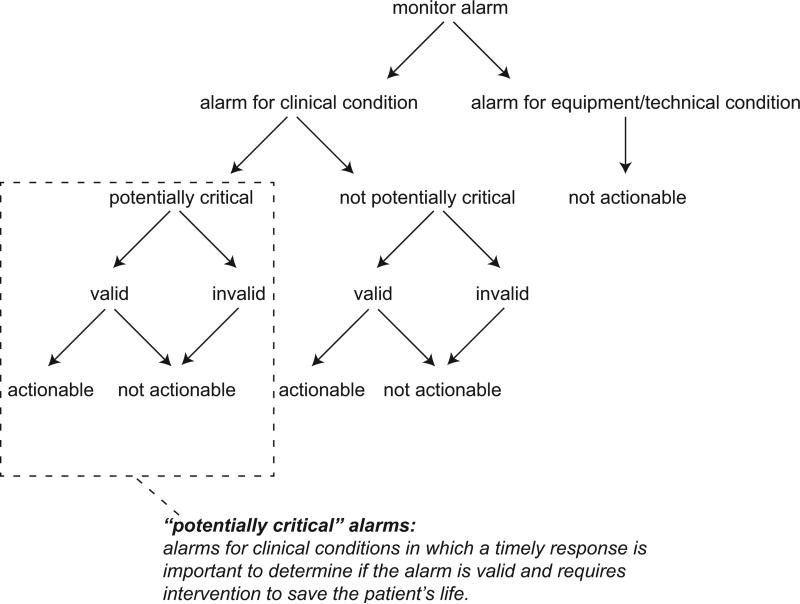
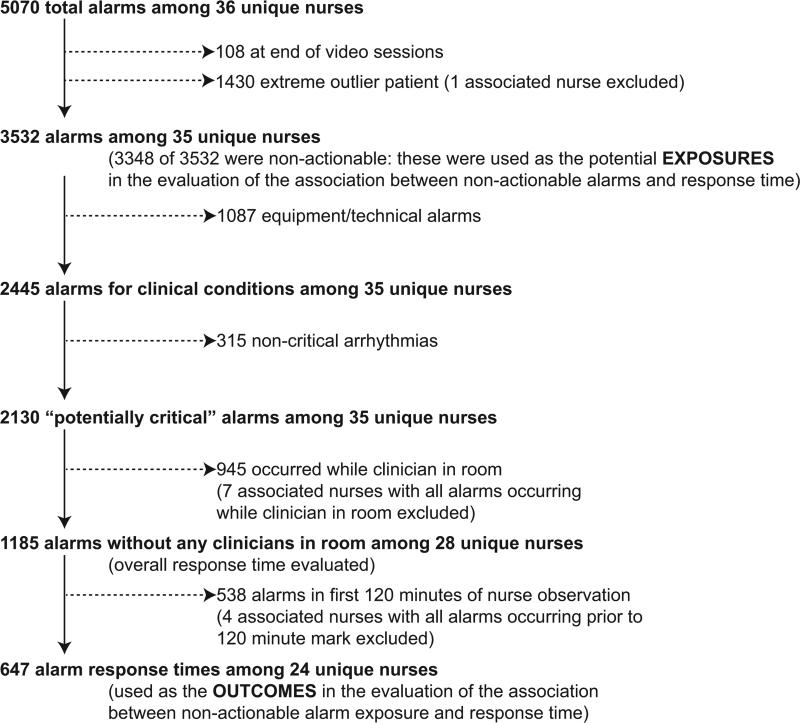
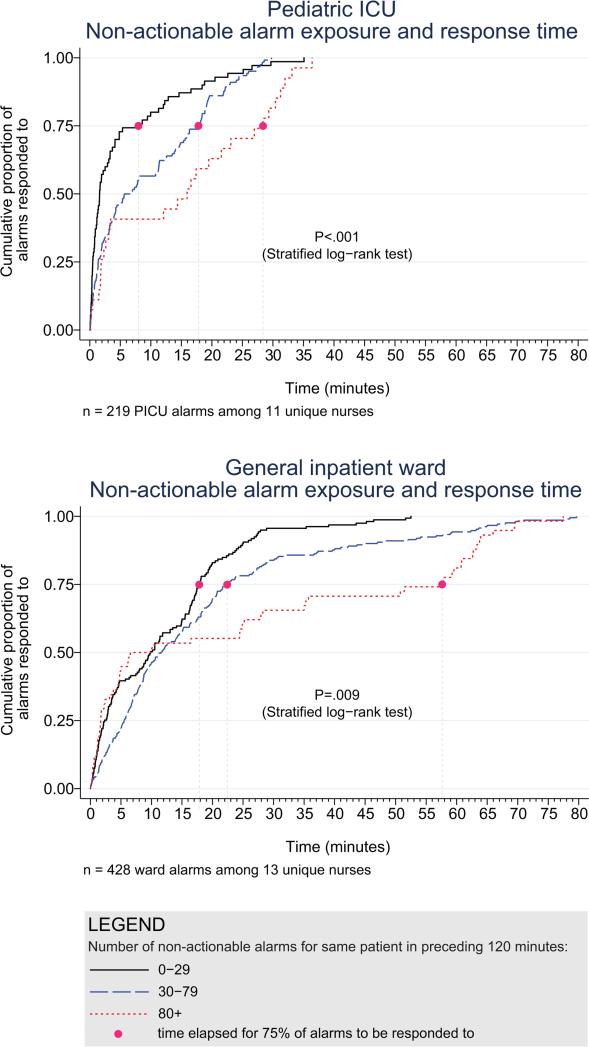
Measurements: Actionable alarms were defined as correctly identifying physiologic status and warranting clinical intervention or consultation. We measured response time to alarms occurring while there were no clinicians in the patient's room. We evaluated the association between the number of nonactionable alarms the patient had in the preceding 120 minutes (categorized as 0-29, 30-79, or 80+ alarms) and response time to subsequent alarms in the same patient using a log-rank test that accounts for within-nurse clustering.
Results: We observed 36 nurses for 210 hours with 5070 alarms; 87.1% of PICU and 99.0% of ward clinical alarms were nonactionable. Kaplan-Meier plots showed incremental increases in response time as the number of nonactionable alarms in the preceding 120 minutes increased (log-rank test stratified by nurse P < 0.001 in PICU, P = 0.009 in the ward).
Conclusions: Most alarms were nonactionable, and response time increased as nonactionable alarm exposure increased. Alarm fatigue could explain these findings. Future studies should evaluate the simultaneous influence of workload and other factors that can impact response time.
© 2015 Society of Hospital Medicine.
Figures
Comment in
-
Crying wolf: False alarms and patient safety.J Hosp Med. 2015 Jun;10(6):409-10. doi: 10.1002/jhm.2355. Epub 2015 Apr 15. J Hosp Med. 2015. PMID: 25879176 No abstract available.
References
-
- Lawless ST. Crying wolf: false alarms in a pediatric intensive care unit. Crit Care Med. 1994;22(6):981–5. - PubMed
-
- Tsien CL, Fackler JC. Poor prognosis for existing monitors in the intensive care unit. Crit. Care Med. 1997;25(4):614–619. - PubMed
-
- Biot L, Carry PY, Perdrix JP, Eberhard A, Baconnier P. [Clinical evaluation of alarm efficiency in intensive care]. Ann Fr Anesth Reanim. 2000;19:459–66. - PubMed
-
- Chambrin MC, Ravaux P, Calvelo-Aros D, Jaborska A, Chopin C, Boniface B. Multicentric study of monitoring alarms in the adult intensive care unit (ICU): a descriptive analysis. Intensive Care Med. 1999;25:1360–1366. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
