

The secular trends in the incidence rate and outcomes of out-of-hospital cardiac arrest in Taiwan--a nationwide population-based study
- PMID: 25875921
- PMCID: PMC4398054
- DOI: 10.1371/journal.pone.0122675
The secular trends in the incidence rate and outcomes of out-of-hospital cardiac arrest in Taiwan--a nationwide population-based study
Abstract
Objective: This study investigated the trends in incidence and mortality of out-of-hospital cardiac arrest (OHCA), as well as factors associated with OHCA outcomes in Taiwan.
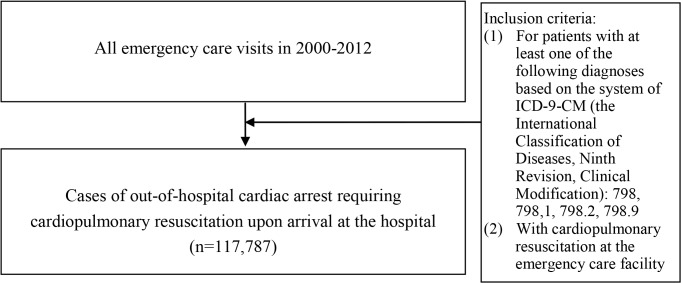
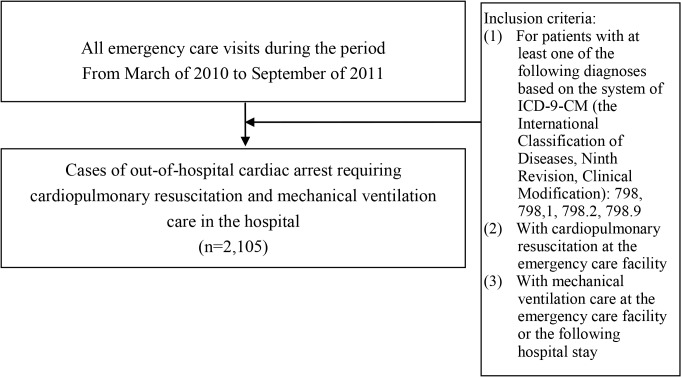
Methods: Our study included OHCA patients requiring cardiopulmonary resuscitation (CPR) upon arrival at the hospital. We used national time-series data on annual OHCA incidence rates and mortality rates from 2000 to 2012, and individual demographic and clinical data for all OHCA patients requiring mechanical ventilation (MV) care from March of 2010 to September of 2011. Analytic techniques included the time-series regression and the logistic regression.
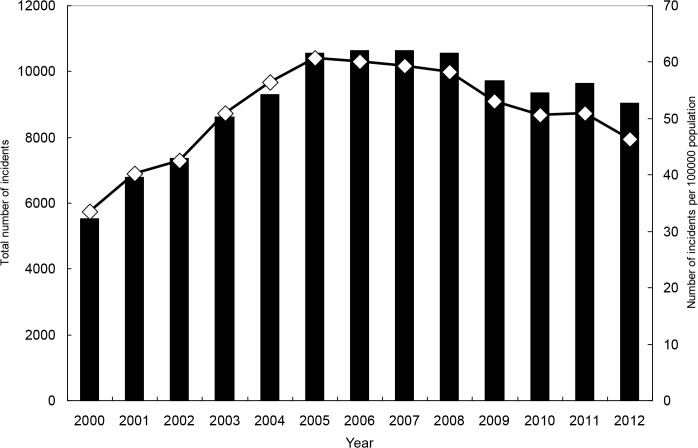
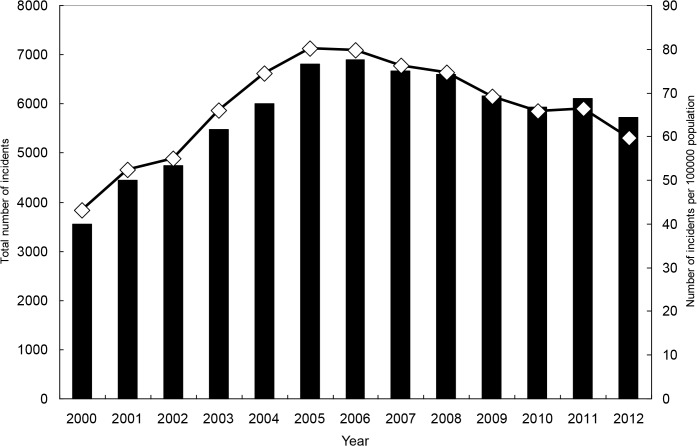
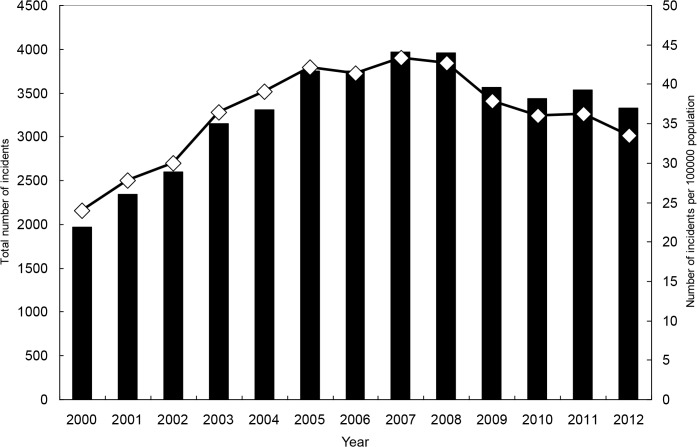
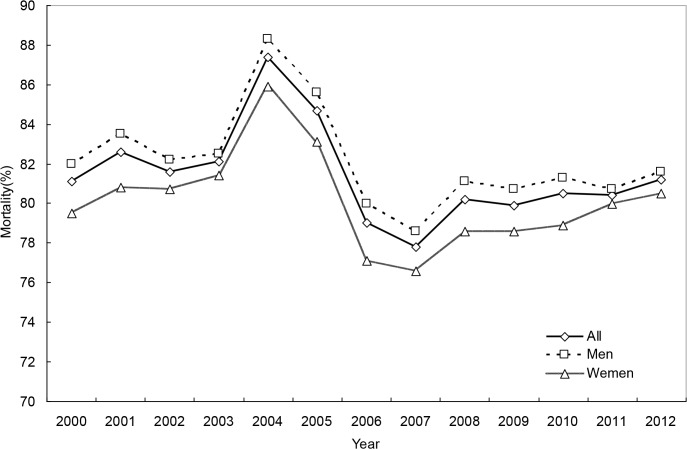
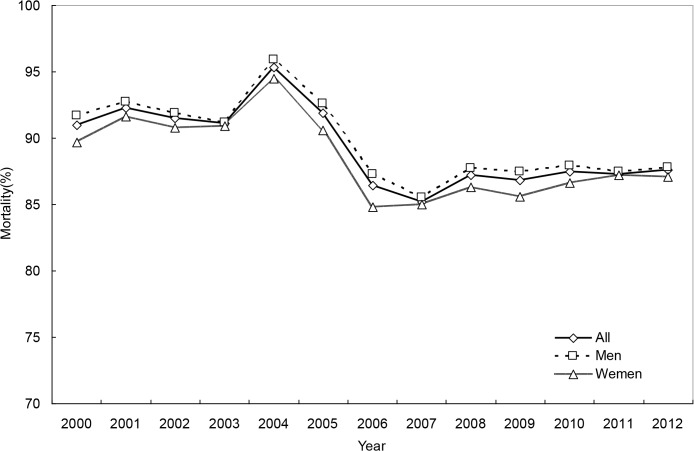
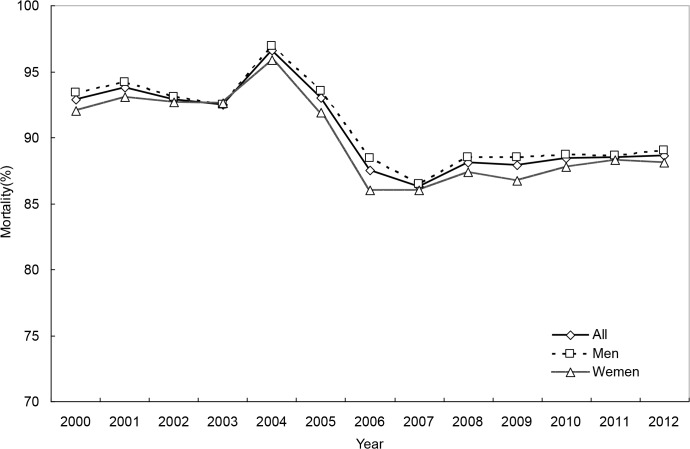
Results: There were 117,787 OHCAs in total. The overall incidence rate during the 13 years was 51.1 per 100,000 persons, and the secular trend indicates a sharp increase in the early 2000s and a decrease afterwards. The trend in mortality was also curvilinear, revealing a substantial increase in the early 2000s, a subsequent steep decline and finally a modest increase. Both the 30-day and 180-day mortality rates had a long-term decreasing trend over the period (p<0.01). For both incidence and mortality rates, a significant second-order autoregressive effect emerged. Among OHCA patients with MV, 1-day, 30-day and 180-day mortality rates were 31.3%, 75.8%, and 86.0%, respectively. In this cohort, older age, the female gender, and a Charlson comorbidity index score ≥ 2 were associated with higher 180-day mortality; patients delivered to regional hospitals and those residing in non-metropolitan areas had higher death risk.
Conclusions: Overall, both the 30-day and the 180-day mortality rates after OHCA had a long-term decreasing trend, while the 1-day mortality had no long-term decline. Among OHCA patients requiring MV, those delivered to regional hospitals and those residing in non-metropolitan areas tended to have higher mortality, suggesting a need for effort to further standardize and improve in-hospital care across hospitals and to advance pre-hospital care in non-metropolitan areas.
Conflict of interest statement
Figures
References
-
- Atwood C, Eisenberg MS, Herlitz J, Rea TD (2005) Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation 67: 75–80. - PubMed
-
- Rea TD, Eisenberg MS, Sinibaldi G, White RD (2004) Incidence of EMS-treated out-of-hospital cardiac arrest in the United States. Resuscitation 63: 17–24. - PubMed
-
- de Vreede-Swagemakers JJ, Gorgels AP, Dubois-Arbouw WI, van Ree JW, Daemen MJ, Houben LG, et al. (1997) Out-of-hospital cardiac arrest in the 1990’s: a population-based study in Maastricht area on incidence, characteristics and survival. J Am Coll Cardiol 30: 1500–1505. - PubMed
-
- Cobb LA, Fanhrenbruch CE, Olsufka M, Copass MK (2002) Changing incidence of out-of-hospital ventricular fibrillation, 1980–2000. JAMA 288: 3008–3013. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
