

Complications After Mastectomy and Immediate Breast Reconstruction for Breast Cancer: A Claims-Based Analysis
- PMID: 25876011
- PMCID: PMC4824182
- DOI: 10.1097/SLA.0000000000001177
Complications After Mastectomy and Immediate Breast Reconstruction for Breast Cancer: A Claims-Based Analysis
Abstract
Objective: To evaluate complications after postmastectomy breast reconstruction, particularly in the setting of adjuvant radiotherapy.
Background: Most studies of complications after breast reconstruction have been conducted at centers of excellence; relatively little is known about complication rates in irradiated patients treated in the broader community. This information is relevant for decision making in patients with breast cancer.
Methods: Using the claims-based MarketScan database, we described complications in 14,894 women undergoing mastectomy for breast cancer from 1998 to 2007 and who underwent immediate autologous reconstruction (n = 2637), immediate implant-based reconstruction (n = 3007), or no reconstruction within the first 2 postoperative years (n = 9250). We used a generalized estimating equation to evaluate associations between complications and radiotherapy over time.
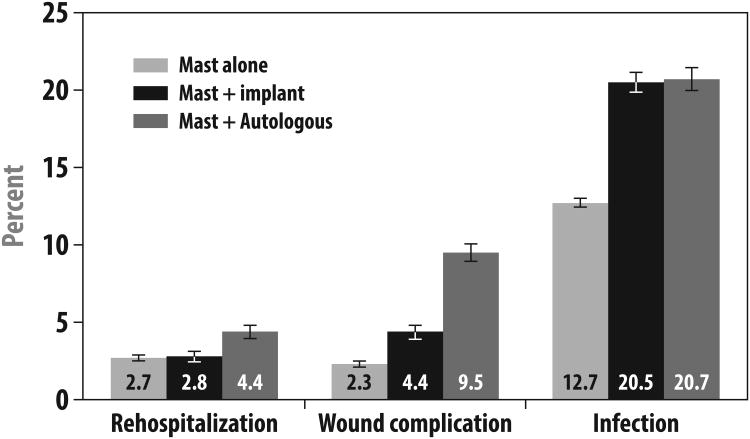
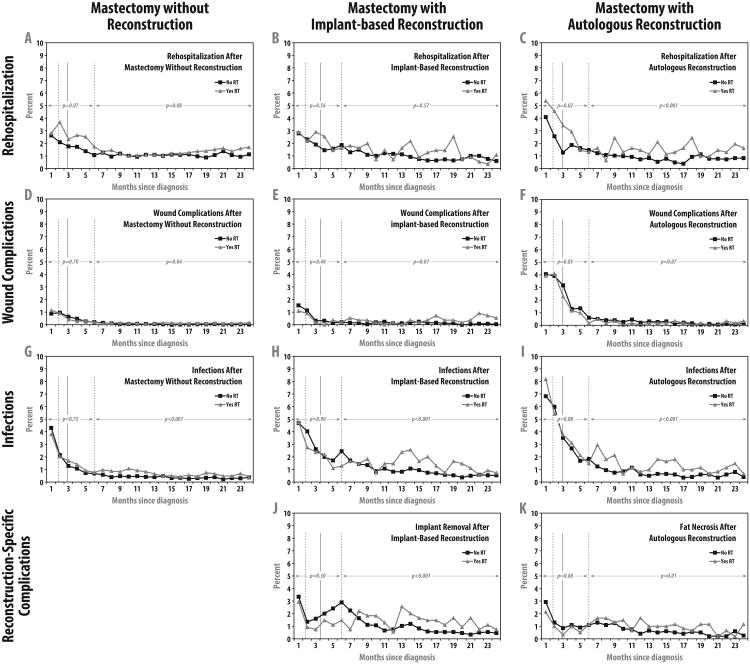
Results: Wound complications were diagnosed within the first 2 postoperative years in 2.3% of patients without reconstruction, 4.4% patients with implants, and 9.5% patients with autologous reconstruction (P < 0.001). Infection was diagnosed within the first 2 postoperative years in 12.7% of patients without reconstruction, 20.5% with implants, and 20.7% with autologous reconstruction (P < 0.001). A total of 5219 (35%) women received radiation. Radiation was not associated with infection in any surgical group within the first 6 months but was associated with an increased risk of infection in months 7 to 24 in all 3 groups (each P < 0.001). In months 7 to 24, radiation was associated with higher odds of implant removal in patients with implant reconstruction (odds ratio = 1.48; P < 0.001) and fat necrosis in those with autologous reconstruction (odds ratio = 1.55; P = 0.01).
Conclusions: Complication risks after immediate breast reconstruction differ by approach. Radiation therapy seems to modestly increase certain risks, including infection and implant removal.
Figures
Comment in
-
Complications After Mastectomy and Immediate Breast Reconstruction for Breast Cancer: How Does the Community Compare?Ann Surg. 2016 Feb;263(2):228-9. doi: 10.1097/SLA.0000000000001584. Ann Surg. 2016. PMID: 26655925 No abstract available.
References
-
- Alderman AK, McMahon L, Jr, Wilkins EG. The national utilization of immediate and early delayed breast reconstruction and the effect of sociodemographic factors. Plast Reconstr Surg. 2003;111:695–703. - PubMed
-
- Reuben BC, Manwaring J, Neumayer LA. Recent trends and predictors in immediate breast reconstruction after mastectomy in the United States. Am J Surg. 2009;198:237–243. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
