Adrenal myelolipoma: Controversies in its management
- PMID: 25878407
- PMCID: PMC4397562
- DOI: 10.4103/0970-1591.152807
Adrenal myelolipoma: Controversies in its management
Abstract
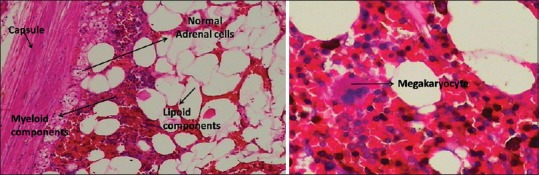
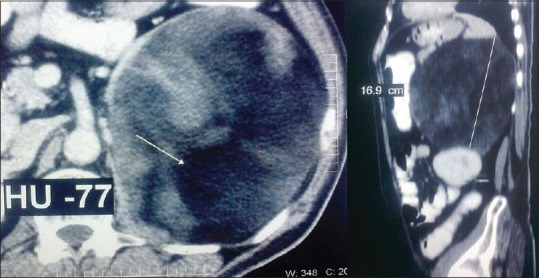
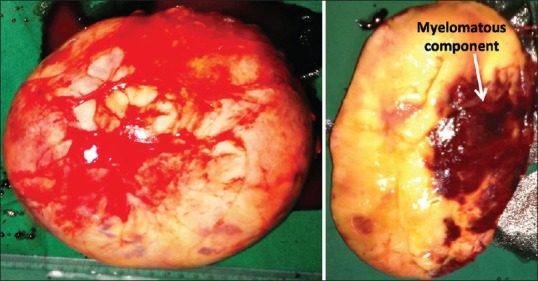
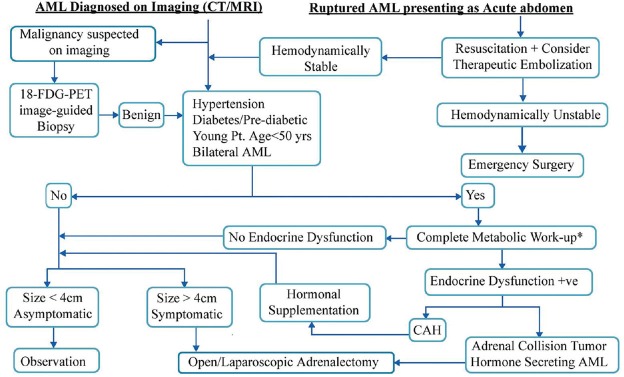
Adrenal myelolipomas (AMLs) are rare, benign neoplasms of the adrenal gland with varied clinical presentations. The rarity of these tumors precludes any case-controlled or randomized study into their management. The available literature is limited to case reports and short series from referral centers. This review is an effort to put the available literature into perspective such that clinical decision making can be done with some clarity. The PubMed and Cochrane databases were searched with key words Adrenal Myelolipoma, Adrenal Incidentaloma (AI) and Adrenal Collision Tumor (ACT). From over 1300 search results, 547 relevant publications dating from 1954 to 2014 were reviewed. Details of about 1231 AMLs in the indexed literature were analyzed. Increasing usage of imaging studies has significantly increased the discovery of AMLs. Although AMLs are benign tumors, those measuring larger than 6 cm are prone to rupture and hemorrhage. Thorough endocrine work-up may benefit a selected group of patients, especially those who are hypertensive, diabetic/pre-diabetic, young patients (<50 years) and those with bilateral AML. Regular observation is needed for AML patients who are being treated non-operatively, as many of them may require surgery during follow-up. Although the AACE/AAES guidelines for AI (2009) exclude AML from mandatory metabolic work-up for a newly discovered AI, we feel that a significant number of patients with AML would benefit from metabolic work-up. In the literature, endocrine dysfunction in AML is 7% as compared with 11% in AI. Endocrine dysfunction in AML is probably underdiagnosed.
Keywords: Adrenal collision tumors; adrenal incidentaloma; adrenal myelolipoma; adrenalectomy.
Conflict of interest statement
Figures
References
-
- Feng C, Jiang H, Ding Q, Wen H. Adrenal myelolipoma: A mingle of progenitor cells. Med Hypotheses. 2013;80:819–22. - PubMed
-
- Bishop E, Eble JN, Cheng L, Wang M, Chase DR, Orazi A, et al. Adrenal myelolipomas show nonrandom X- chromosome inactivation in hematopoietic elements and fat: Support for a clonal origin of myelolipomas. Am J Surg Pathol. 2006;30:838–43. - PubMed
-
- Schulte KM, Heinze M, Mengel M, Scheuring S, Köhrer K, Röher HD. Complete sequencing and mRNA expression analysis of the MEN-I gene in adrenal myelolipoma. Horm Metab Res. 2000;32:169–73. - PubMed
-
- Adleff V, Rácz K, Tóth M, Varga I, Bezzegh A, Gláz E. P 53 protein and its messenger ribonucleic acid in human adrenal tumors. J Endocrinol Invest. 1998;21:753–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources