

Immune profile of IgA-dominant diffuse proliferative glomerulonephritis
- PMID: 25878780
- PMCID: PMC4379348
- DOI: 10.1093/ckj/sfu090
Immune profile of IgA-dominant diffuse proliferative glomerulonephritis
Abstract
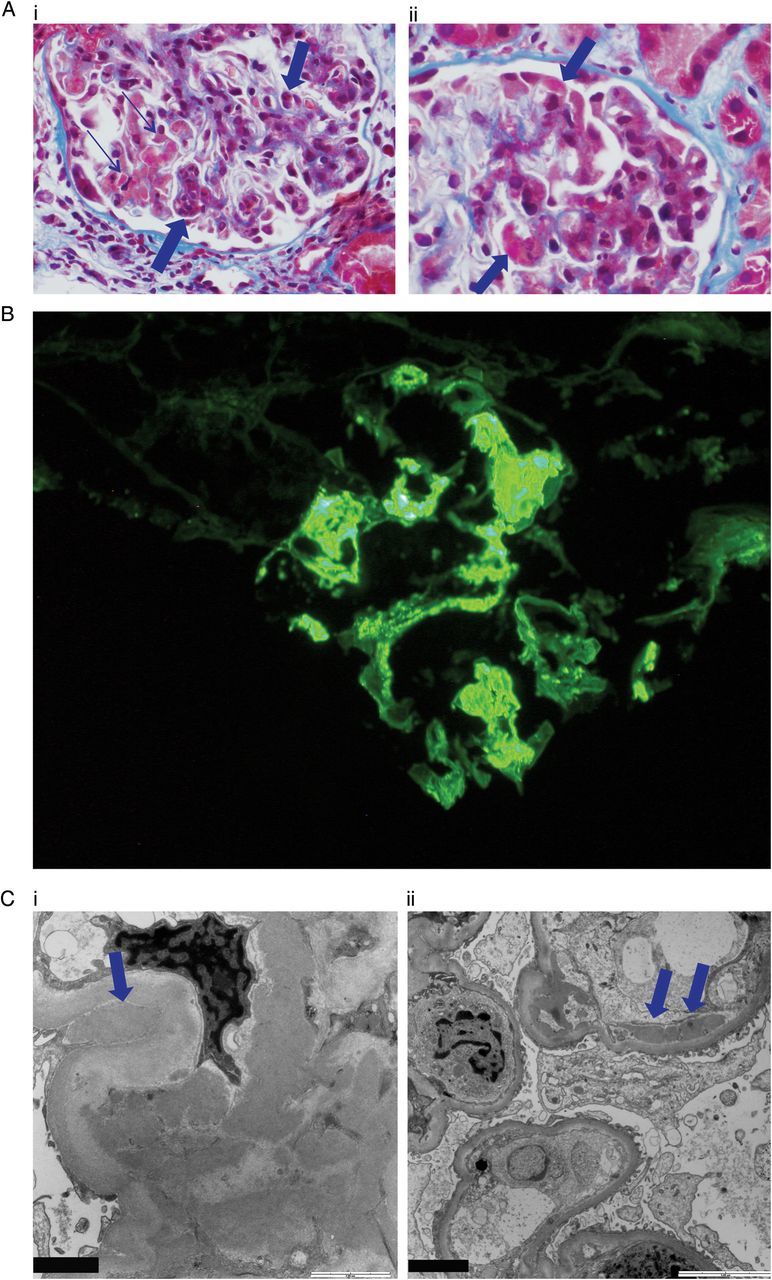
The diagnosis of IgA-dominant post-infectious glomerulonephritis (PIGN) may be challenging, as it must be differentiated from that of active IgA nephropathy. Predominant clinicopathologic features of IgA-dominant PIGN substantially overlap with those of active IgA nephropathy. Here, we present a case of a 67-year-old woman with rapidly rising serum creatinine, proteinuria and severe hypertension. The kidney biopsy findings included some features of IgA-dominant PIGN while others were more consistent with classical IgA nephropathy. We describe this patient's immune profile at the time of acute kidney injury and review the literature regarding differentiation of the two entities.
Keywords: IgA; IgA dominant post-infectious glomerulonephritis; IgA nephropathy.
Figures
Similar articles
-
A rare case of Immunoglobulin A dominant post-infectious glomerulonephritis (IgA PIGN) in a young patient.BMC Nephrol. 2022 Oct 17;23(1):333. doi: 10.1186/s12882-022-02965-7. BMC Nephrol. 2022. PMID: 36253737 Free PMC article.
-
IgA-dominant post-infectious glomerulonephritis presenting as a fatal pulmonary-renal syndrome.Int J Nephrol Renovasc Dis. 2015 Aug 5;8:77-81. doi: 10.2147/IJNRD.S84061. eCollection 2015. Int J Nephrol Renovasc Dis. 2015. PMID: 26347210 Free PMC article.
-
Discrimination between postinfectious IgA-dominant glomerulonephritis and idiopathic IgA nephropathy.Ren Fail. 2010 Jun;32(5):572-7. doi: 10.3109/08860221003753331. Ren Fail. 2010. PMID: 20486840
-
Post-infectious glomerulonephritis.Paediatr Int Child Health. 2017 Nov;37(4):240-247. doi: 10.1080/20469047.2017.1369642. Epub 2017 Sep 11. Paediatr Int Child Health. 2017. PMID: 28891413 Review.
-
Histology and immunohistology of IgA nephropathy.J Nephrol. 2005 Nov-Dec;18(6):676-80. J Nephrol. 2005. PMID: 16358224 Review.
Cited by
-
IgA-dominant Infection-related Glomerulonephritis in India: A Single-center Experience.Indian J Nephrol. 2017 Nov-Dec;27(6):435-439. doi: 10.4103/ijn.IJN_337_16. Indian J Nephrol. 2017. PMID: 29217879 Free PMC article.
-
Rapidly progressive IgA nephropathy with membranoproliferative glomerulonephritis-like lesions in an elderly man following the third dose of an mRNA COVID-19 vaccine: a case report.BMC Nephrol. 2023 Apr 24;24(1):108. doi: 10.1186/s12882-023-03169-3. BMC Nephrol. 2023. PMID: 37095451 Free PMC article.
-
IgA-Dominant Infection-Associated Glomerulonephritis Following SARS-CoV-2 Infection.Viruses. 2021 Mar 31;13(4):587. doi: 10.3390/v13040587. Viruses. 2021. PMID: 33807151 Free PMC article.
-
Clinicopathological and prognostic study of IgA-dominant postinfectious glomerulonephritis.BMC Nephrol. 2021 Jul 5;22(1):248. doi: 10.1186/s12882-021-02462-3. BMC Nephrol. 2021. PMID: 34225678 Free PMC article.
-
IgA-dominant infection-associated glomerulonephritis in the pediatric population.Pediatr Nephrol. 2022 Mar;37(3):593-600. doi: 10.1007/s00467-021-05245-y. Epub 2021 Aug 28. Pediatr Nephrol. 2022. PMID: 34453602
References
-
- Nasr SH, Fidler ME, Valeri AM, et al. Postinfectious glomerulonephritis in the elderly. J Am Soc Nephrol. 2011;22:187–195. - PubMed
-
- Haas M, Racusen LC, Bagnasco SM. IgA-dominant postinfectious glomerulonephritis: a report of 13 cases with common ultrastructural features. Hum Pathol. 2008;39:1309–1316. - PubMed
-
- Nasr SH, D'Agati VD. IgA-dominant postinfectious glomerulonephritis: a new twist on an old disease. Nephron Clin Pract. 2011;119:c18–c26. - PubMed
-
- Yoshikawa N, Ito H, Nakahara C, et al. Glomerular electron-dense deposits in childhood IgA nephropathy. Virchows Arch A Pathol Anat Histopathol. 1985;406:33–43. - PubMed
-
- Nasr SH, Markowitz GS, Whelan JD, et al. IgA-dominant acute poststaphylococcal glomerulonephritis complicating diabetic nephropathy. Hum Pathol. 2003;34:1235–1241. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
