

Simultaneous cranioplasty and subdural-peritoneal shunting for contralateral symptomatic subdural hygroma following decompressive craniectomy
- PMID: 25879062
- PMCID: PMC4386681
- DOI: 10.1155/2015/518494
Simultaneous cranioplasty and subdural-peritoneal shunting for contralateral symptomatic subdural hygroma following decompressive craniectomy
Abstract
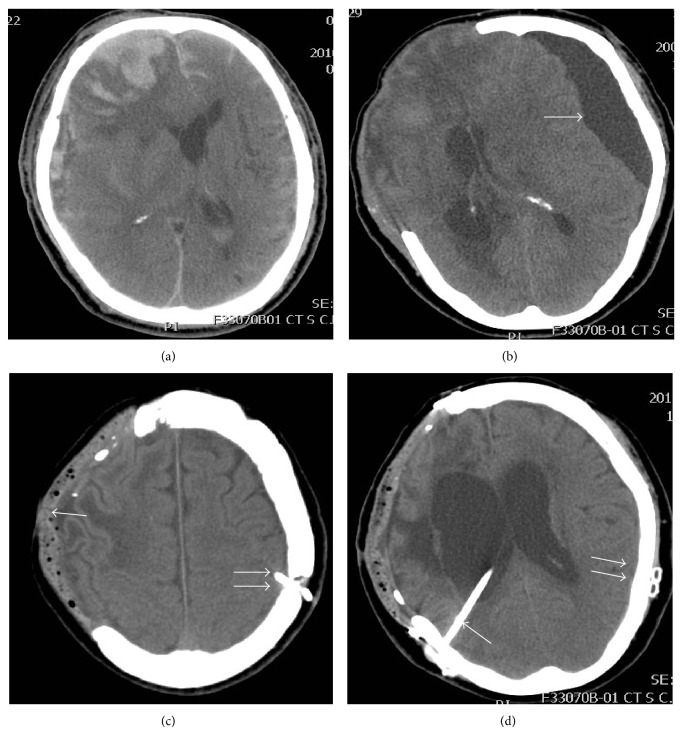
Background: Contralateral subdural hygroma caused by decompressive craniectomy tends to combine with external cerebral herniation, causing neurological deficits.
Material and methods: Nine patients who underwent one-stage, simultaneous cranioplasty and contralateral subdural-peritoneal shunting were included in this study. Clinical outcome was assessed by Glasgow Outcome Scale as well as Glasgow Coma Scale, muscle power scoring system, and complications.
Results: Postoperative computed tomography scans demonstrated completely resolved subdural hygroma and reversed midline shifts, indicating excellent outcome. Among these 9 patients, 4 patients (44%) had improved GOS following the proposed surgery. Four out of 4 patients with lethargy became alert and orientated following surgical intervention. Muscle strength improved significantly 5 months after surgery in 7 out of 7 patients with weakness. Two out of 9 patients presented with drowsiness due to hydrocephalus at an average time of 65 days after surgery. Double gradient shunting is useful to eliminate the respective hydrocephalus and contralateral subdural hygroma.
Conclusion: The described surgical technique is effective in treating symptomatic contralateral subdural hygroma following decompressive craniectomy and is associated with an excellent structural and functional outcome. However, subdural-peritoneal shunting plus cranioplasty thoroughly resolves the subdural hygroma collection, which might deteriorate the cerebrospinal fluid circulation, leading to hydrocephalus.
Figures
References
-
- Timofeev I., Kirkpatrick P. J., Corteen E., et al. Decompressive craniectomy in traumatic brain injury: outcome following protocol-driven therapy. Acta Neurochirurgica. 2006;96:11–16. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
