

Guideline-concordant antibiotic prescribing for pediatric outpatients with otitis media, community-acquired pneumonia, and skin and soft tissue infections in a large multispecialty healthcare system
- PMID: 25879084
- PMCID: PMC4394205
Guideline-concordant antibiotic prescribing for pediatric outpatients with otitis media, community-acquired pneumonia, and skin and soft tissue infections in a large multispecialty healthcare system
Abstract
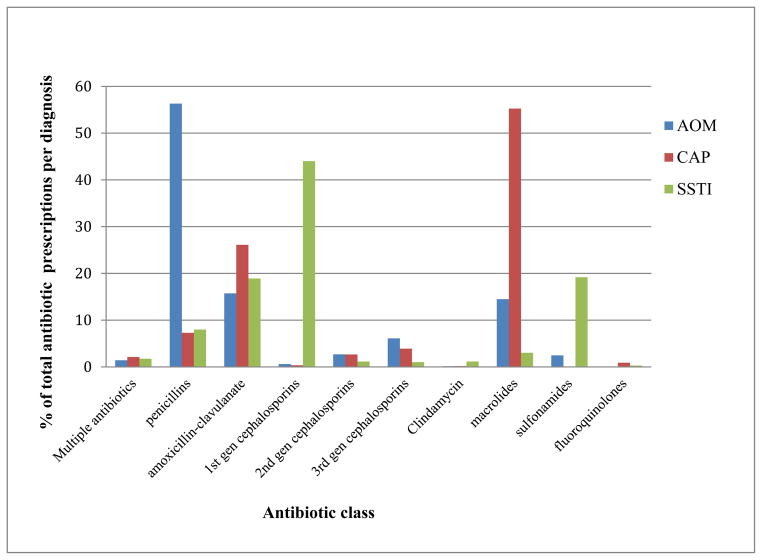
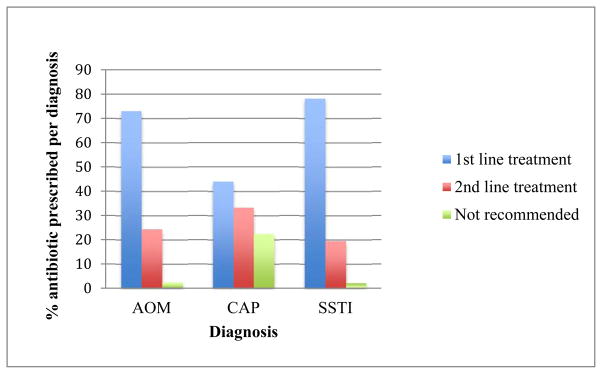
Antibiotics are commonly prescribed in pediatric outpatient settings; however, efforts to decrease inappropriate use have largely focused on inpatients. We obtained baseline metrics to identify conditions that may benefit from establishment of outpatient antimicrobial stewardship interventions (ASP). We evaluated rates and appropriateness of antibiotic prescribing for children with acute otitis media (AOM), community acquired pneumonia (CAP), and skin and soft tissue infections (SSTI) in ambulatory settings within a large healthcare system in the US Midwest. We retrospectively reviewed 77,821 visits and associated diagnostic codes for children less than 17 years seen in ambulatory settings within our health system from August 1, 2009 to July 31, 2010. We measured rates of antibiotic prescribing by location, provider type, patient age, and diagnosis, and assessed concordance with treatment guidelines for AOM, CAP, and SSTI. AOM, CAP, and SSTI comprised about 1/3 of all infections in the study population. Antibiotics were prescribed in 14,543 (18.7%) visits. Antibiotic prescribing rates were 1.1 to 1.2 times higher among Emergency Room (ER) providers compared to Pediatricians and Family Physicians. Antibiotics prescribed for AOM and SSTI were concordant with guidelines in approximately 97% of cases. In contrast, 47% of antibiotics prescribed for treatment of CAP in children < 5 years old were macrolides, which are not recommended first line therapy for CAP in this age group. Antibiotic prescribing for pediatric outpatients within our health system is not guideline-concordant for treatment of CAP.
Keywords: Antimicrobial stewardship; Otitis Media; Pediatrics; Pneumonia; Skin and soft tissue infections.
Figures
Similar articles
-
The long and the short of pediatric emergency department antibiotic prescribing: A retrospective observational study.Am J Emerg Med. 2024 Jan;75:131-136. doi: 10.1016/j.ajem.2023.10.052. Epub 2023 Nov 5. Am J Emerg Med. 2024. PMID: 37950980
-
Ambulatory Antibiotic Prescribing for Children with Pneumonia After Publication of National Guidelines: A Cross-Sectional Retrospective Study.Infect Dis Ther. 2020 Mar;9(1):69-76. doi: 10.1007/s40121-019-00276-3. Epub 2019 Nov 27. Infect Dis Ther. 2020. PMID: 31776843 Free PMC article.
-
Variability in Antibiotic Prescribing for Upper Respiratory Illnesses by Provider Specialty.J Pediatr. 2018 Dec;203:76-85.e8. doi: 10.1016/j.jpeds.2018.07.044. Epub 2018 Sep 5. J Pediatr. 2018. PMID: 30195553
-
Pediatric acute otitis media: the case for delayed antibiotic treatment.J Emerg Med. 2007 Apr;32(3):279-84. doi: 10.1016/j.jemermed.2006.07.029. Epub 2007 Feb 23. J Emerg Med. 2007. PMID: 17394992 Review.
-
It's about the patients: Practical antibiotic stewardship in outpatient settings in the United States.Front Med (Lausanne). 2022 Jul 27;9:901980. doi: 10.3389/fmed.2022.901980. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35966853 Free PMC article. Review.
Cited by
-
Discordance Among Antibiotic Prescription Guidelines Reflects a Lack of Clear Best Practices.Open Forum Infect Dis. 2020 Dec 22;8(1):ofaa571. doi: 10.1093/ofid/ofaa571. eCollection 2021 Jan. Open Forum Infect Dis. 2020. PMID: 33447636 Free PMC article.
-
Recent Developments in Pediatric Community-Acquired Pneumonia.Curr Infect Dis Rep. 2016 May;18(5):14. doi: 10.1007/s11908-016-0521-1. Curr Infect Dis Rep. 2016. PMID: 26960931
-
Appropriate Use of Antibiotic and Principles of Antimicrobial Stewardship in Children.Children (Basel). 2023 Apr 17;10(4):740. doi: 10.3390/children10040740. Children (Basel). 2023. PMID: 37189989 Free PMC article.
-
Antibiotic Prescribing for Children in United States Emergency Departments: 2009-2014.Pediatrics. 2019 Feb;143(2):e20181056. doi: 10.1542/peds.2018-1056. Epub 2019 Jan 8. Pediatrics. 2019. PMID: 30622156 Free PMC article.
-
Outpatient Pediatric Antibiotic Use: a Systematic Review.Curr Infect Dis Rep. 2019 Mar 20;21(4):14. doi: 10.1007/s11908-019-0673-x. Curr Infect Dis Rep. 2019. PMID: 30895479 Free PMC article. Review.
References
-
- Hersh AL, Shapiro DJ, Pavia AT, Shah SS. Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics. 2011;128(6):1053–61. - PubMed
-
- Halasa NB, Griffin MR, Zhu Y, Edwards KM. Decreased number of antibiotic prescriptions in office-based settings from 1993 to 1999 in children less than five years of age. The Pediatr Infect Dis J. 2002;21(11):1023–8. - PubMed
-
- Dooling KL, Shapiro DJ, Van Beneden C, Hersh AL, Hicks LA. Overprescribing and inappropriate antibiotic selection for children with pharyngitis in the United States, 1997–2010. JAMA Pediatrics. 2014;168(11):1073–4. - PubMed
-
- MacDougall C, Powell JP, Johnson CK, Edmond MB, Polk RE. Hospital and community fluoroquinolone use and resistance in Staphylococcus aureus and Escherichia coli in 17 US hospitals. Clin Infect Dis. 2005;41(4):435–40. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous