

Paracetamol therapy and outcome of critically ill patients: a multicenter retrospective observational study
- PMID: 25879463
- PMCID: PMC4411740
- DOI: 10.1186/s13054-015-0865-1
Paracetamol therapy and outcome of critically ill patients: a multicenter retrospective observational study
Abstract
Introduction: In this study, we aimed to examine the association between paracetamol administration in the intensive care unit (ICU) and mortality in critically ill patients.
Methods: We conducted a multicenter retrospective observational study in four ICUs. We obtained information on paracetamol use, body temperature, demographic, clinical and outcome data from each hospital's clinical information system and admissions and discharges database. We performed statistical analysis to assess the association between paracetamol administration and hospital mortality.
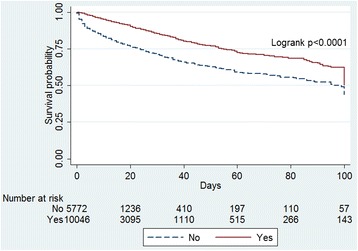
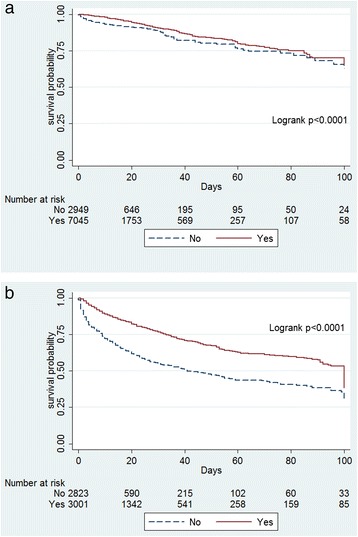
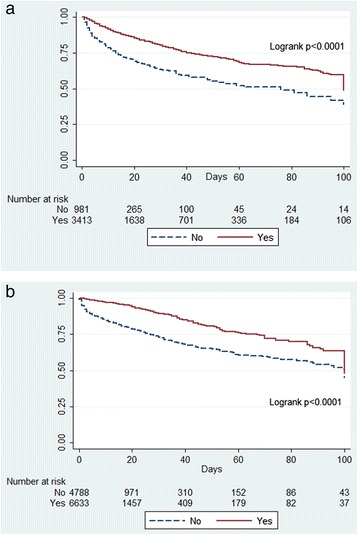
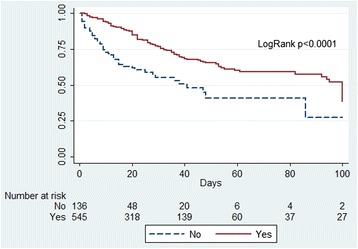
Results: We studied 15,818 patients with 691,348 temperature measurements at 4 ICUs. Of these patients, 10,046 (64%) received at least 1 g of paracetamol. Patients who received paracetamol had lower in-hospital mortality (10% vs. 20%, P <0.001), and survivors were more likely to have received paracetamol (66% vs. 46%; P <0.001). However, patients treated with paracetamol were also more likely to be admitted to the ICU after surgery (70% vs. 51%; P <0.001) and/or after elective surgery (55% vs. 37%; P <0.001). In multivariate logistic regression analysis including a propensity score for paracetamol treatment, we found a significant and independent association between the use of paracetamol and reduced in-hospital mortality (adjusted odds ratio =0.60 (95% confidence interval (CI), 0.53 to 0.68), P <0.001). Cox proportional hazards analysis showed that patients who received paracetamol also had a significantly longer time to death (adjusted hazard ratio =0.51 (95% CI, 0.46 to 0.56), P <0.001). The association between paracetamol and decreased mortality and/or time to death was broadly consistent across surgical and medical patients. It remained present after adjusting for paracetamol administration as a time-dependent variable. However, when such time-dependent analysis was performed, the association of paracetamol with outcome lost statistical significance in the presence of fever and suspected infection and in patients in the lower tertiles of Acute Physiology and Chronic Health Evaluation II scores.
Conclusions: Paracetamol administration is common in the ICU and appears to be independently associated with reduced in-hospital mortality and time to death after adjustment for multiple potential confounders and propensity score. This association, however, was modified by the presence of fever, suspected infection and lesser illness severity and may represent the effect of indication bias.
Figures
References
-
- Jefferies S, Saxena M, Young P. Paracetamol in critical illness: a review. Crit Care Resusc. 2012;14:74–80. - PubMed
-
- Daly FFS, Fountain JS, Murray L, Graudins A, Buckley NA. Guidelines for the management of paracetamol poisoning in Australia and New Zealand—explanation and elaboration: a consensus statement from clinical toxicologists consulting to the Australasian poisons information centres. Med J Aust. 2008;188:296–301. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
