

Neurally adjusted ventilatory assist and proportional assist ventilation both improve patient-ventilator interaction
- PMID: 25879592
- PMCID: PMC4355459
- DOI: 10.1186/s13054-015-0763-6
Neurally adjusted ventilatory assist and proportional assist ventilation both improve patient-ventilator interaction
Abstract
Introduction: The objective was to compare the impact of three assistance levels of different modes of mechanical ventilation; neurally adjusted ventilatory assist (NAVA), proportional assist ventilation (PAV), and pressure support ventilation (PSV) on major features of patient-ventilator interaction.
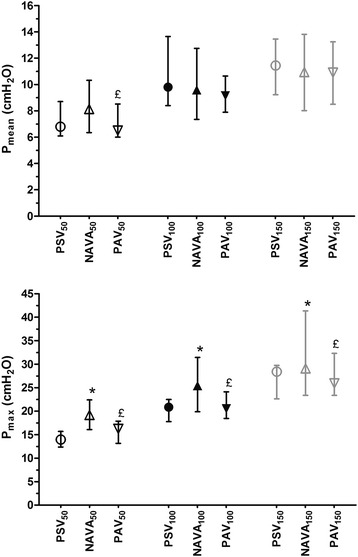
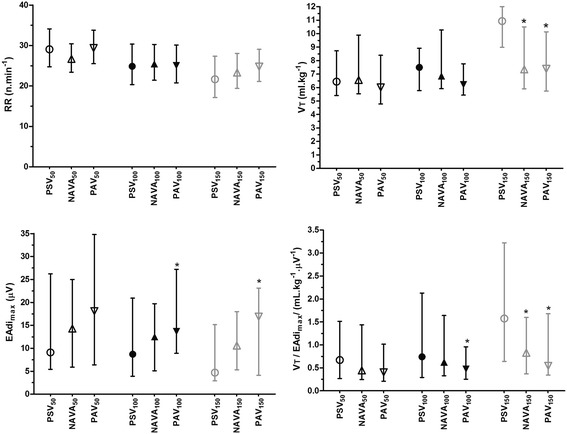
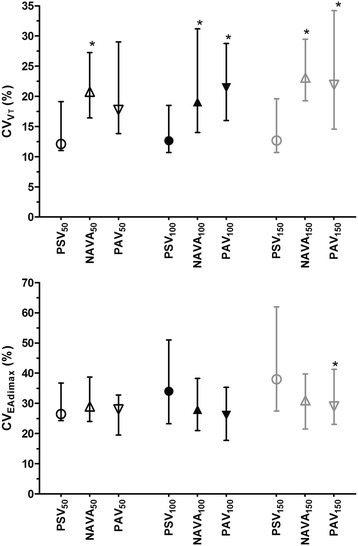
Methods: PSV, NAVA, and PAV were set to obtain a tidal volume (VT) of 6 to 8 ml/kg (PSV₁₀₀, NAVA₁₀₀, and PAV₁₀₀) in 16 intubated patients. Assistance was further decreased by 50% (PSV₅₀, NAVA₅₀, and PAV₅₀) and then increased by 50% (PSV₁₅₀, NAVA₁₅₀, and PAV₁₅₀) with all modes. The three modes were randomly applied. Airway flow and pressure, electrical activity of the diaphragm (EAdi), and blood gases were measured. VT, peak EAdi, coefficient of variation of VT and EAdi, and the prevalence of the main patient-ventilator asynchronies were calculated.
Results: PAV and NAVA prevented the increase of VT with high levels of assistance (median 7.4 (interquartile range (IQR) 5.7 to 10.1) ml/kg and 7.4 (IQR, 5.9 to 10.5) ml/kg with PAV₁₅₀ and NAVA₁₅₀ versus 10.9 (IQR, 8.9 to 12.0) ml/kg with PSV₁₅₀, P <0.05). EAdi was higher with PAV than with PSV at level₁₀₀ and level₁₅₀. The coefficient of variation of VT was higher with NAVA and PAV (19 (IQR, 14 to 31)% and 21 (IQR 16 to 29)% with NAVA₁₀₀ and PAV₁₀₀ versus 13 (IQR 11 to 18)% with PSV₁₀₀, P <0.05). The prevalence of ineffective triggering was lower with PAV and NAVA than with PSV (P <0.05), but the prevalence of double triggering was higher with NAVA than with PAV and PSV (P <0.05).
Conclusions: PAV and NAVA both prevent overdistention, improve neuromechanical coupling, restore the variability of the breathing pattern, and decrease patient-ventilator asynchrony in fairly similar ways compared with PSV. Further studies are needed to evaluate the possible clinical benefits of NAVA and PAV on clinical outcomes.
Trial registration: Clinicaltrials.gov NCT02056093 . Registered 18 December 2013.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
